

Diastolic dysfunction in men with severe obstructive sleep apnea syndrome but without cardiovascular or oxidative stress-related comorbidities
- PMID: 31566076
- PMCID: PMC6769220
- DOI: 10.1177/1753466619880076
Diastolic dysfunction in men with severe obstructive sleep apnea syndrome but without cardiovascular or oxidative stress-related comorbidities
Abstract
Background: We aimed to evaluate whether the severity of obstructive sleep apnea syndrome (OSAS) per se affects the prevalence of left ventricular (LV) diastolic dysfunction in patients without comorbidities.
Methods: A total of 42 patients with first-diagnosed severe OSAS [apnea-hypopnea index (AHI) > 30] and 25 controls (AHI < 5), having been referred for snoring to the Sleep Laboratory Department of our tertiary Hospital, were enrolled in the study. Inclusion criteria were absence of any cardiovascular or oxidative stress-related comorbidities, and age between 20 and 70 years. Clinical, laboratory, echocardiographic, and polysomnographic data were recorded prospectively. Diastolic dysfunction diagnosis and grading was based on 2016 ASE/EACVI recommendations.
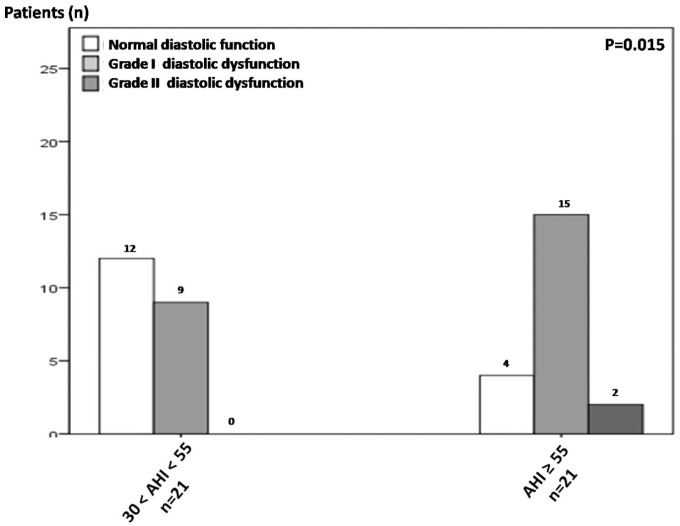
Results: Severe OSAS was associated with significantly increased prevalence and degree of diastolic dysfunction (26/42; 61.9%) compared with controls (7/25; 28%) (p = 0.007). AHI ⩾ 55 (dichotomous value of severe OSAS subset) was also characterized by greater prevalence and degree of diastolic dysfunction compared with 30 < AHI < 55 patients (p = 0.015). In the severe OSAS subset, age >45 years-old, height <1.745 m, body-mass index (BMI) >27.76 kg m-2, OSAS severity (AHI > 57.35), oxidative stress (overnight reduction of reduced to oxidized glutathione ratio < 18.44%), and BMI/height ratio > 16.155 kg m-3 (an index describing 'dense', short-heavy patients) presented significant diagnostic utility in identifying diastolic dysfunction in ROC-curve analysis (0.697 ⩾ AUC ⩾ 0.855, 0.001 ⩽ p ⩽ 0.018). In binary logistic regression model, advanced age (OR 1.23, 95% CI 1.025-1.477; p = 0.026) and AHI (OR 1.123, 95% CI 1.007-1.253; p = 0.036) showed independent association with diastolic dysfunction in severe OSAS.
Conclusions: The present prospective study may suggest that severe OSAS is significantly associated with LV diastolic dysfunction; OSAS clinical severity exerts a positive influence on (and possibly constitutes an independent risk factor of) LV diastolic dysfunction. The reviews of this paper are available via the supplementary material section.
Keywords: GSH; GSSG; comorbidity; diastolic dysfunction; obstructive sleep apnea syndrome; oxidative stress.
Conflict of interest statement
Figures


Similar articles
-
Left ventricular diastolic dysfunction in obstructive sleep apnoea syndrome by an echocardiographic standardized approach: An observational study.Arch Cardiovasc Dis. 2015 Oct;108(10):480-90. doi: 10.1016/j.acvd.2015.03.006. Epub 2015 Jun 8. Arch Cardiovasc Dis. 2015. PMID: 26068195
-
Influence and predicting variables of obstructive sleep apnea on cardiac function and remodeling in patients without congestive heart failure.J Clin Sleep Med. 2014 Jan 15;10(1):57-64. doi: 10.5664/jcsm.3360. J Clin Sleep Med. 2014. PMID: 24426821 Free PMC article.
-
Oxidative stress in patients with obstructive sleep apnea syndrome.Sleep Breath. 2013 May;17(2):549-55. doi: 10.1007/s11325-012-0718-y. Epub 2012 May 18. Sleep Breath. 2013. PMID: 22610662
-
Technical report: diagnosis and management of childhood obstructive sleep apnea syndrome.Pediatrics. 2002 Apr;109(4):e69. doi: 10.1542/peds.109.4.e69. Pediatrics. 2002. PMID: 11927742 Review.
-
Consequences of obstructive sleep apnoea syndrome on left ventricular geometry and diastolic function.Arch Cardiovasc Dis. 2016 Aug-Sep;109(8-9):494-503. doi: 10.1016/j.acvd.2016.02.011. Epub 2016 Jun 22. Arch Cardiovasc Dis. 2016. PMID: 27344377 Review.
Cited by
-
Role of Oxidative Stress in the Occurrence and Development of Cognitive Dysfunction in Patients with Obstructive Sleep Apnea Syndrome.Mol Neurobiol. 2024 Aug;61(8):5083-5101. doi: 10.1007/s12035-023-03899-3. Epub 2023 Dec 30. Mol Neurobiol. 2024. PMID: 38159196 Review.
-
A novel diastolic dysfunction score: A proposed diagnostic predictor for left ventricular dysfunction in obese population.Narra J. 2025 Apr;5(1):e1564. doi: 10.52225/narra.v5i1.1564. Epub 2025 Apr 17. Narra J. 2025. PMID: 40352170 Free PMC article.
-
Analysis of vasoactive and oxidative stress indicators for evaluating the efficacy of continuous positive airway pressure, and relation of vasoactive and oxidative stress indicators and cardiac function in obstructive sleep Apnea Syndrome patients.J Med Biochem. 2024 Apr 23;43(2):200-208. doi: 10.5937/jomb0-42944. J Med Biochem. 2024. PMID: 38699699 Free PMC article.
-
Relationships between Obstructive Sleep Apnea Syndrome and cardiovascular risk in a naïve population of southern Italy.Int J Clin Pract. 2021 Dec;75(12):e14952. doi: 10.1111/ijcp.14952. Epub 2021 Oct 18. Int J Clin Pract. 2021. PMID: 34610197 Free PMC article.
-
Changes in Left Heart Geometry, Function, and Blood Serum Biomarkers in Patients with Obstructive Sleep Apnea after Treatment with Continuous Positive Airway Pressure.Medicina (Kaunas). 2022 Oct 24;58(11):1511. doi: 10.3390/medicina58111511. Medicina (Kaunas). 2022. PMID: 36363468 Free PMC article.
References
-
- Hung J, Whitford EG, Parsons RW, et al. Association of sleep apnoea with myocardial infarction in men. Lancet 1990; 336: 261–264. - PubMed
-
- Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med 2002; 165: 1217–1239. - PubMed
-
- Yaggi HK, Concato J, Kernan WN, et al. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med 2005; 353: 2034–2041. - PubMed
-
- Bradley TD, Floras JS. Sleep apnea and heart failure: part I: obstructive sleep apnea. Circulation 2003; 107: 1671–1678. - PubMed
-
- Wachtell K, Palmieri V, Gerdts E, et al. Prognostic significance of left ventricular diastolic dysfunction in patients with left ventricular hypertrophy and systemic hypertension (the LIFE Study). Am J Cardiol 2010; 106: 999–1005. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
