

Diastolic dysfunction in men with severe obstructive sleep apnea syndrome but without cardiovascular or oxidative stress-related comorbidities
- PMID: 31566076
- PMCID: PMC6769220
- DOI: 10.1177/1753466619880076
Diastolic dysfunction in men with severe obstructive sleep apnea syndrome but without cardiovascular or oxidative stress-related comorbidities
Abstract
Background: We aimed to evaluate whether the severity of obstructive sleep apnea syndrome (OSAS) per se affects the prevalence of left ventricular (LV) diastolic dysfunction in patients without comorbidities.
Methods: A total of 42 patients with first-diagnosed severe OSAS [apnea-hypopnea index (AHI) > 30] and 25 controls (AHI < 5), having been referred for snoring to the Sleep Laboratory Department of our tertiary Hospital, were enrolled in the study. Inclusion criteria were absence of any cardiovascular or oxidative stress-related comorbidities, and age between 20 and 70 years. Clinical, laboratory, echocardiographic, and polysomnographic data were recorded prospectively. Diastolic dysfunction diagnosis and grading was based on 2016 ASE/EACVI recommendations.
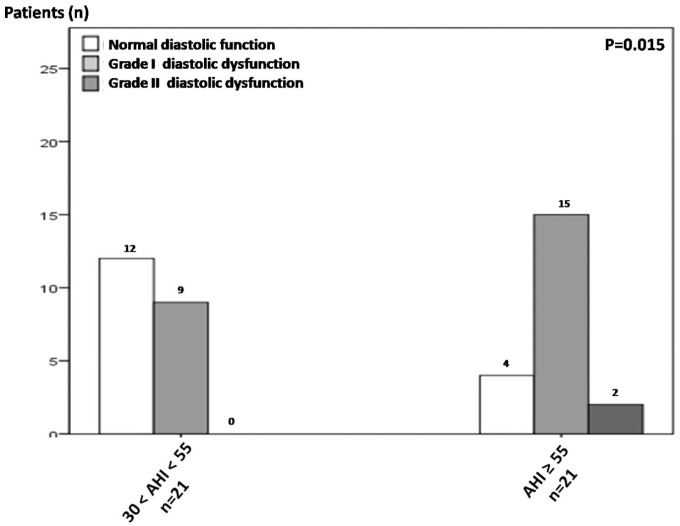
Results: Severe OSAS was associated with significantly increased prevalence and degree of diastolic dysfunction (26/42; 61.9%) compared with controls (7/25; 28%) (p = 0.007). AHI ⩾ 55 (dichotomous value of severe OSAS subset) was also characterized by greater prevalence and degree of diastolic dysfunction compared with 30 < AHI < 55 patients (p = 0.015). In the severe OSAS subset, age >45 years-old, height <1.745 m, body-mass index (BMI) >27.76 kg m-2, OSAS severity (AHI > 57.35), oxidative stress (overnight reduction of reduced to oxidized glutathione ratio < 18.44%), and BMI/height ratio > 16.155 kg m-3 (an index describing 'dense', short-heavy patients) presented significant diagnostic utility in identifying diastolic dysfunction in ROC-curve analysis (0.697 ⩾ AUC ⩾ 0.855, 0.001 ⩽ p ⩽ 0.018). In binary logistic regression model, advanced age (OR 1.23, 95% CI 1.025-1.477; p = 0.026) and AHI (OR 1.123, 95% CI 1.007-1.253; p = 0.036) showed independent association with diastolic dysfunction in severe OSAS.
Conclusions: The present prospective study may suggest that severe OSAS is significantly associated with LV diastolic dysfunction; OSAS clinical severity exerts a positive influence on (and possibly constitutes an independent risk factor of) LV diastolic dysfunction. The reviews of this paper are available via the supplementary material section.
Keywords: GSH; GSSG; comorbidity; diastolic dysfunction; obstructive sleep apnea syndrome; oxidative stress.
Conflict of interest statement
Figures


References
-
- Hung J, Whitford EG, Parsons RW, et al. Association of sleep apnoea with myocardial infarction in men. Lancet 1990; 336: 261–264. - PubMed
-
- Young T, Peppard PE, Gottlieb DJ. Epidemiology of obstructive sleep apnea: a population health perspective. Am J Respir Crit Care Med 2002; 165: 1217–1239. - PubMed
-
- Yaggi HK, Concato J, Kernan WN, et al. Obstructive sleep apnea as a risk factor for stroke and death. N Engl J Med 2005; 353: 2034–2041. - PubMed
-
- Bradley TD, Floras JS. Sleep apnea and heart failure: part I: obstructive sleep apnea. Circulation 2003; 107: 1671–1678. - PubMed
-
- Wachtell K, Palmieri V, Gerdts E, et al. Prognostic significance of left ventricular diastolic dysfunction in patients with left ventricular hypertrophy and systemic hypertension (the LIFE Study). Am J Cardiol 2010; 106: 999–1005. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Molecular Biology Databases
