

A Comparative Modeling Analysis of Risk-Based Lung Cancer Screening Strategies
- PMID: 31566216
- PMCID: PMC7225672
- DOI: 10.1093/jnci/djz164
A Comparative Modeling Analysis of Risk-Based Lung Cancer Screening Strategies
Abstract
Background: Risk-prediction models have been proposed to select individuals for lung cancer screening. However, their long-term effects are uncertain. This study evaluates long-term benefits and harms of risk-based screening compared with current United States Preventive Services Task Force (USPSTF) recommendations.
Methods: Four independent natural history models were used to perform a comparative modeling study evaluating long-term benefits and harms of selecting individuals for lung cancer screening through risk-prediction models. In total, 363 risk-based screening strategies varying by screening starting and stopping age, risk-prediction model used for eligibility (Bach, PLCOm2012, or Lung Cancer Death Risk Assessment Tool [LCDRAT]), and risk threshold were evaluated for a 1950 US birth cohort. Among the evaluated outcomes were percentage of individuals ever screened, screens required, lung cancer deaths averted, life-years gained, and overdiagnosis.
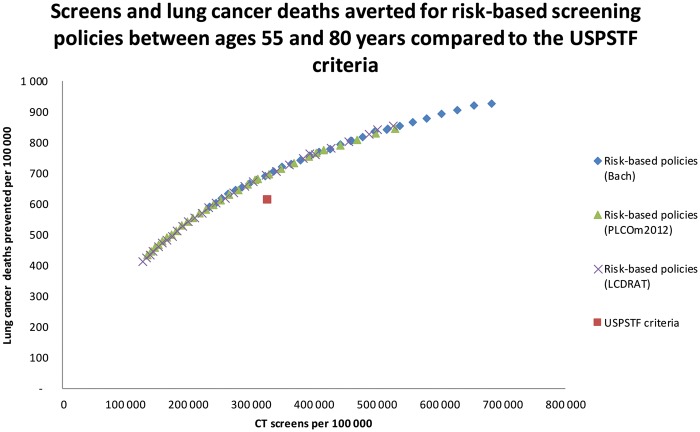
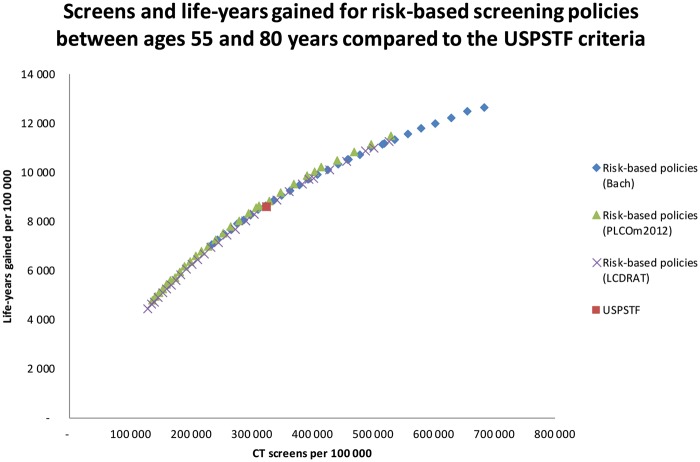
Results: Risk-based screening strategies requiring similar screens among individuals ages 55-80 years as the USPSTF criteria (corresponding risk thresholds: Bach = 2.8%; PLCOm2012 = 1.7%; LCDRAT = 1.7%) averted considerably more lung cancer deaths (Bach = 693; PLCOm2012 = 698; LCDRAT = 696; USPSTF = 613). However, life-years gained were only modestly higher (Bach = 8660; PLCOm2012 = 8862; LCDRAT = 8631; USPSTF = 8590), and risk-based strategies had more overdiagnosed cases (Bach = 149; PLCOm2012 = 147; LCDRAT = 150; USPSTF = 115). Sensitivity analyses suggest excluding individuals with limited life expectancies (<5 years) from screening retains the life-years gained by risk-based screening, while reducing overdiagnosis by more than 65.3%.
Conclusions: Risk-based lung cancer screening strategies prevent considerably more lung cancer deaths than current recommendations do. However, they yield modest additional life-years and increased overdiagnosis because of predominantly selecting older individuals. Efficient implementation of risk-based lung cancer screening requires careful consideration of life expectancy for determining optimal individual stopping ages.
© The Author(s) 2019. Published by Oxford University Press.
Figures
Comment in
-
Basing Eligibility for Lung Cancer Screening on Individualized Risk Calculators Should Save More Lives, but Life Expectancy Matters.J Natl Cancer Inst. 2020 May 1;112(5):429-430. doi: 10.1093/jnci/djz165. J Natl Cancer Inst. 2020. PMID: 31566223 Free PMC article. No abstract available.
References
-
- Moyer VA, on behalf of the U.S. Preventive Services Task Force. Screening for lung cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med. 2014;160(5):330–338. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
