

Multi-institutional Development and External Validation of a Nomogram to Predict Recurrence After Curative Resection of Pancreatic Neuroendocrine Tumors
- PMID: 31567347
- PMCID: PMC8557638
- DOI: 10.1097/SLA.0000000000003579
Multi-institutional Development and External Validation of a Nomogram to Predict Recurrence After Curative Resection of Pancreatic Neuroendocrine Tumors
Abstract
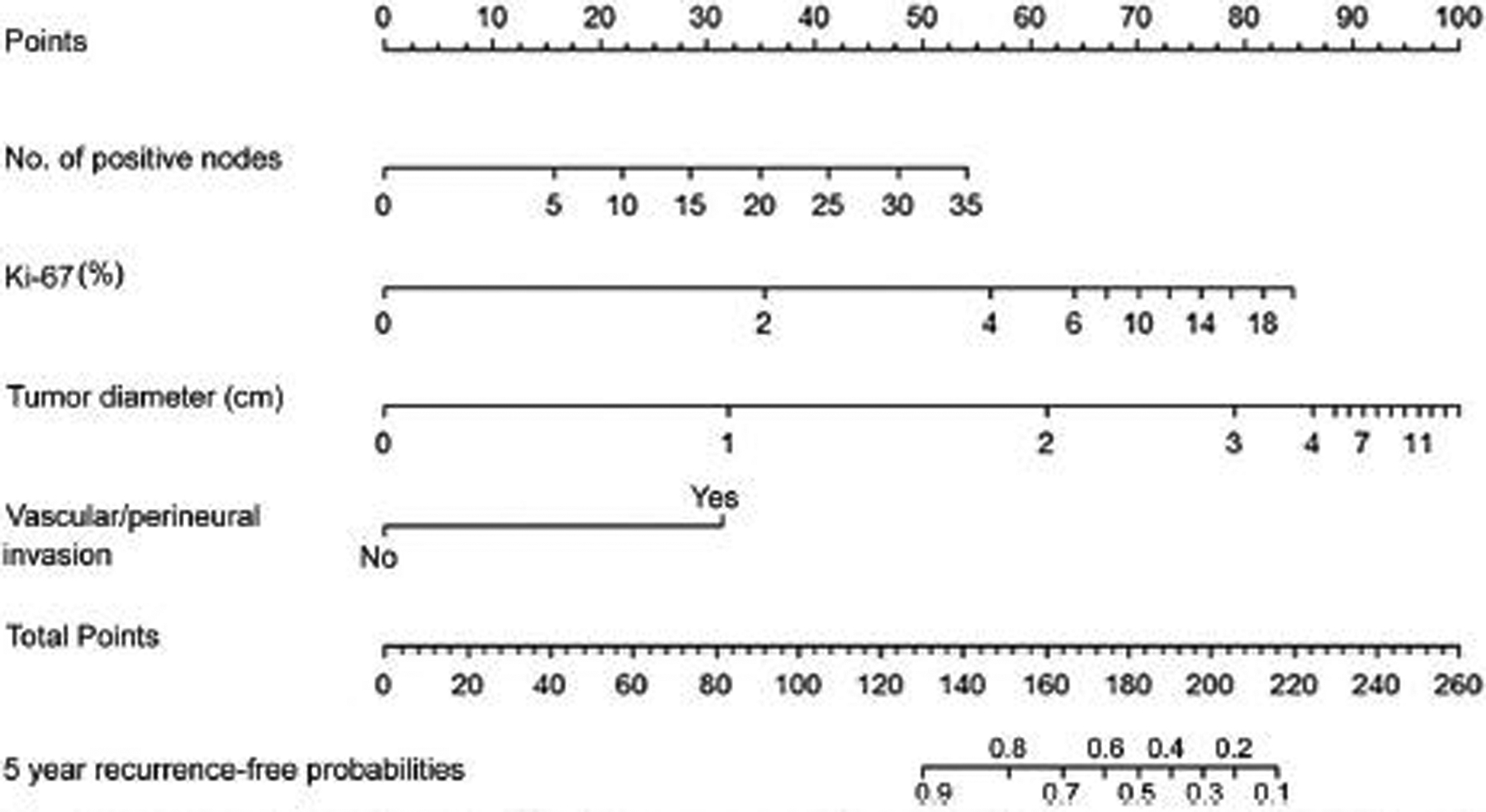
Objective: To develop a nomogram estimating the probability of recurrence free at 5 years after resection for localized grade 1 (G1)/ grade 2 (G2) pancreatic neuroendocrine tumors (PanNETs).
Background: Among patients undergoing resection of PanNETs, approximately 17% experience recurrence. It is not established which patients are at risk, with no consensus on optimal follow-up.
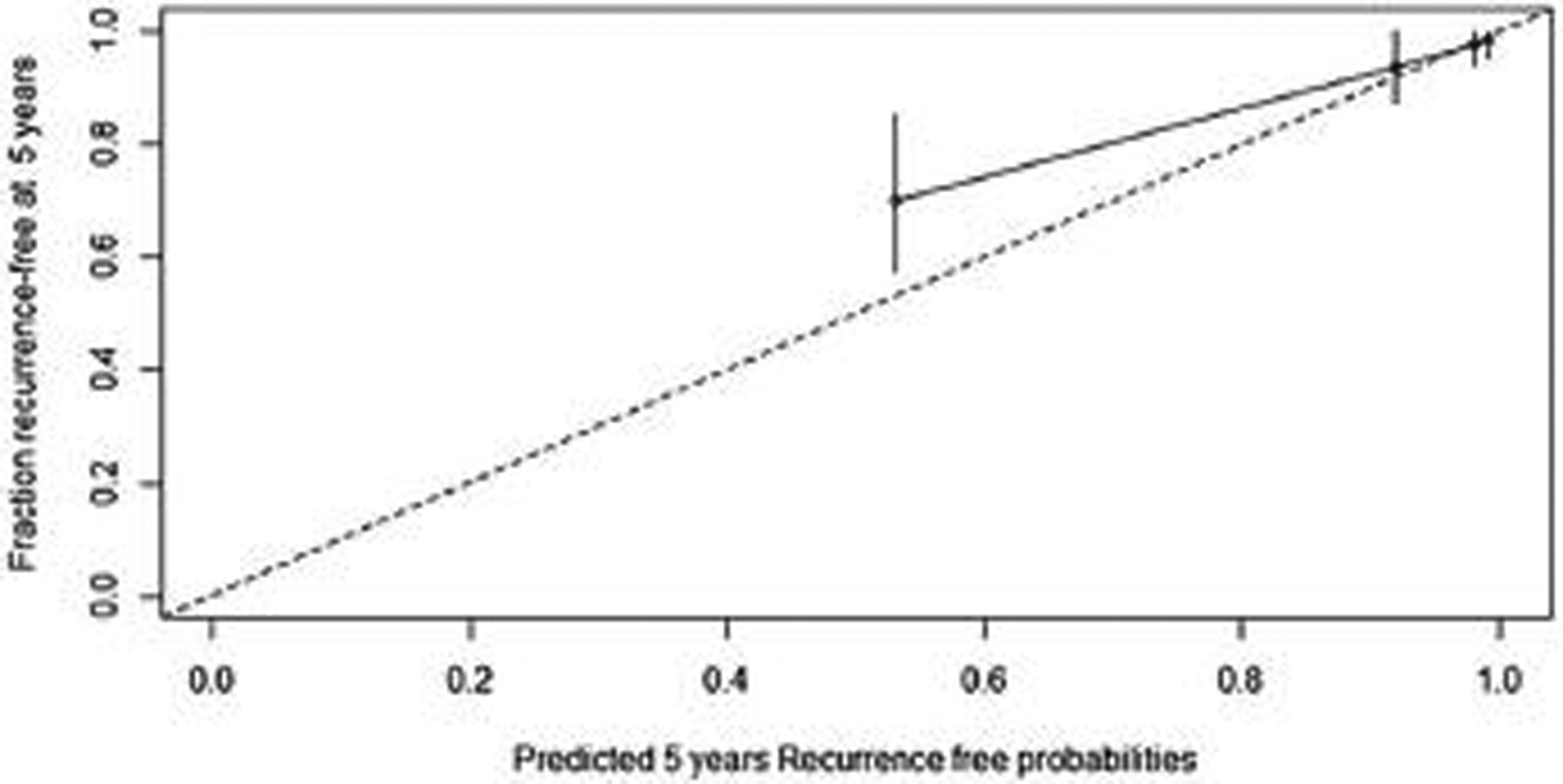
Method: A multi-institutional database of patients with G1/G2 PanNETs treated at 2 institutions was used to develop a nomogram estimating the rate of freedom from recurrence at 5 years after curative resection. A second cohort of patients from 3 additional institutions was used to validate the nomogram. Prognostic factors were assessed by univariate analysis using Cox regression model. The nomogram was internally validated using bootstrap resampling method and on the external cohort. Performance was assessed by concordance index (c-index) and a calibration curve.
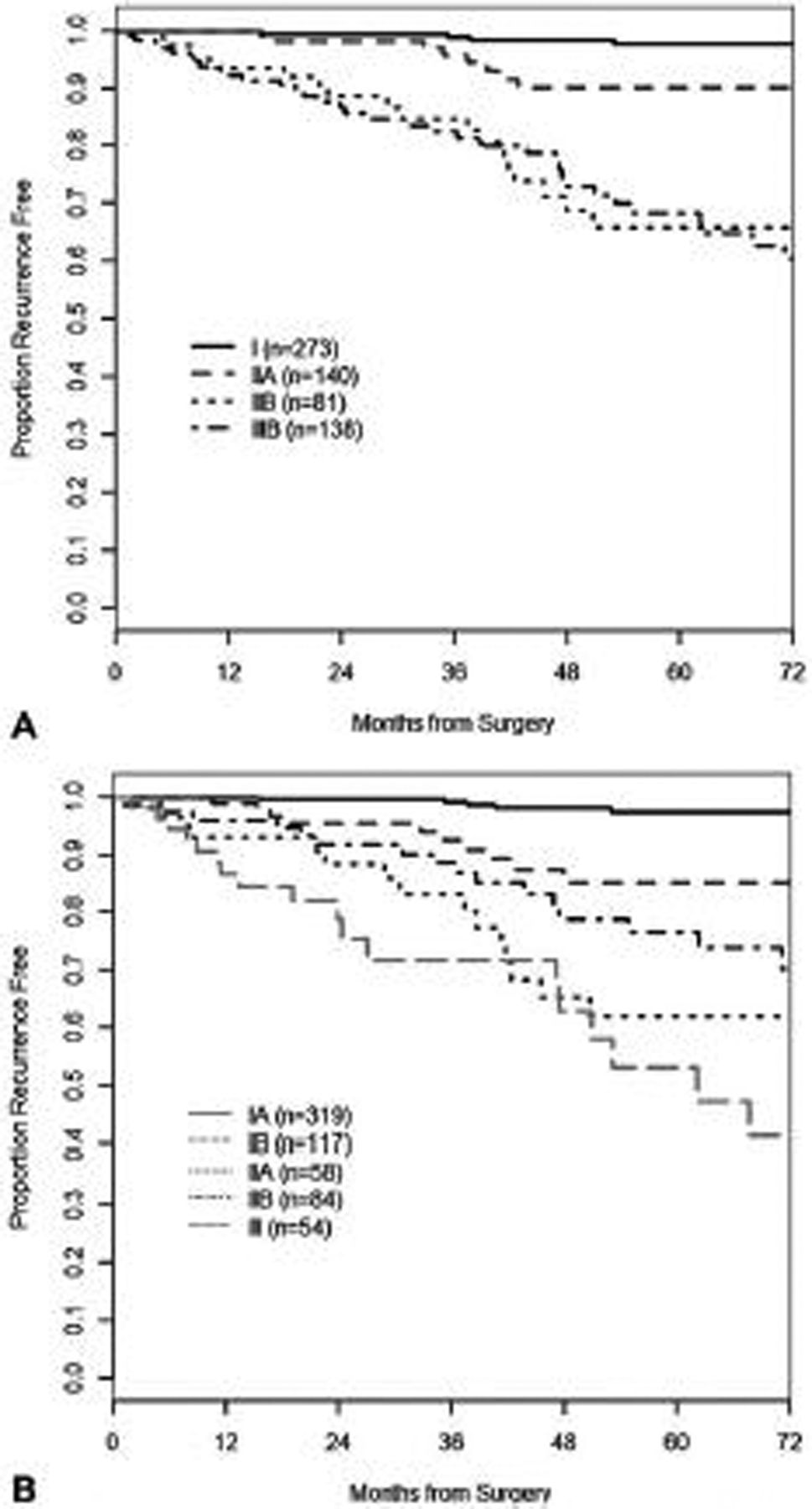
Results: The nomogram was constructed using a cohort of 632 patients. Overall, 68% of PanNETs were G1, the median follow-up was 51 months, and we observed 74 recurrences. Variables included in the nomogram were the number of positive nodes, tumor diameter, Ki-67, and vascular/perineural invasion. The model bias-corrected c-index from the internal validation was 0.85, which was higher than European Neuroendocrine Tumors Society/ American Joint Committee on Cancer 8th staging scheme (c-index 0.76, P = <0.001). On the external cohort of 328 patients, the nomogram c-index was 0.84 (95% confidence interval 0.79-0.88).
Conclusion: Our externally validated nomogram predicts the probability of recurrence-free survival at 5 years after PanNETs curative resection, with improved accuracy over current staging systems. Estimating individual recurrence risk will guide the development of personalized surveillance programs after surgery.
Copyright © 2019 Wolters Kluwer Health, Inc. All rights reserved.
Conflict of interest statement
The authors declare no conflict of interests.
Figures
References
-
- Pulvirenti A, Marchegiani G, Pea A, et al. Clinical implications of the 2016 International Study Group on pancreatic surgery definition and grading of postoperative pancreatic fistula on 775 consecutive pancreatic resections. Ann Surg. 2018;268:1069–1075. - PubMed
-
- Strosberg JR, Cheema A, Weber JM, et al. Relapse-free survival in patients with nonmetastatic, surgically resected pancreatic neuroendocrine tumors. Ann Surg. 2012;256:321–325. - PubMed
-
- Ricci C, Casadei R, Taffurelli G, et al. Is radical surgery always curative in pancreatic neuroendocrine tumors? A cure model survival analysis. Pancreatology. 2018;1–5. - PubMed
-
- Landoni L, Marchegiani G, Pollini T, et al. The evolution of surgical strategies for pancreatic neuroendocrine tumors (Pan-NENs). Ann Surg. 2019;269: 725–732. - PubMed
-
- The International Agency for Research on Cancer. In: Bosman FT, Carneiro F, Hruban RH, Theise N, eds. WHO Classification of Tumours of the Digestive System. 4th ed, World Health Organization; 2010:418.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
