

Papillary thyroid carcinoma with tracheal invasion: A case report
- PMID: 31567939
- PMCID: PMC6756740
- DOI: 10.1097/MD.0000000000017033
Papillary thyroid carcinoma with tracheal invasion: A case report
Abstract
Rationale: Compared with most malignant tumors, papillary thyroid carcinoma (PTC) is usually associated with favorable survival and low recurrence rate. The prognostic factors of PTC include age, sex, tumor size, enlarged lymph nodes, and extrathyroidal extension. Among the extrathyroidal extension, upper aerodigestive tract (ADT) invasion by PTC is a marker of more aggressive tumor behavior, defining a subpopulation of patients at a greater risk of recurrence and death.
Patient concerns: A 61-year-old woman had a cervical mass that was slowly growing for three years. Additionally, she had haemoptysis of 1-year duration. During the month prior to her visit, she had difficulty breathing.
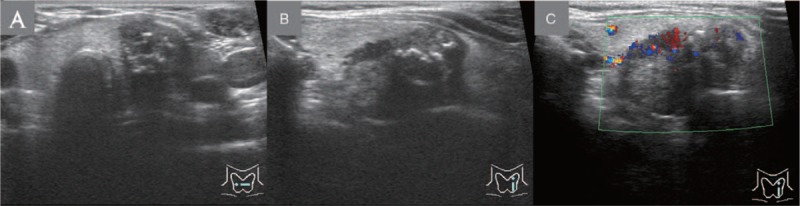
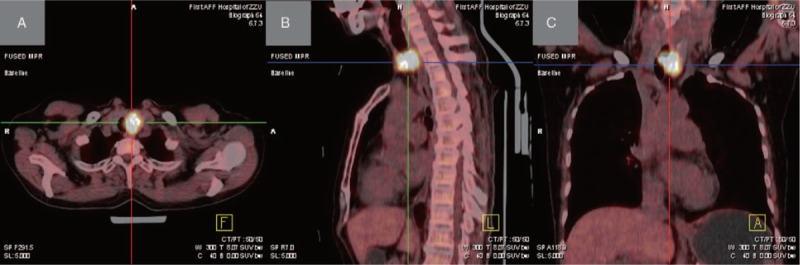
Diagnosis: Neck ultrasonography (US) and thyroid computed tomography (CT) images both showed a well-defined calcified mass on the left lobe of the thyroid gland. Additionally, the thyroid CT revealed that part of the mass protruded into the lumen which resulted in the thickening on the left side of the trachea. Accordingly, her diagnoses were as follows: firstly, a solid mass on the left lobe of the thyroid gland with tracheal compression; and finally, the space-occupying airway lesion.
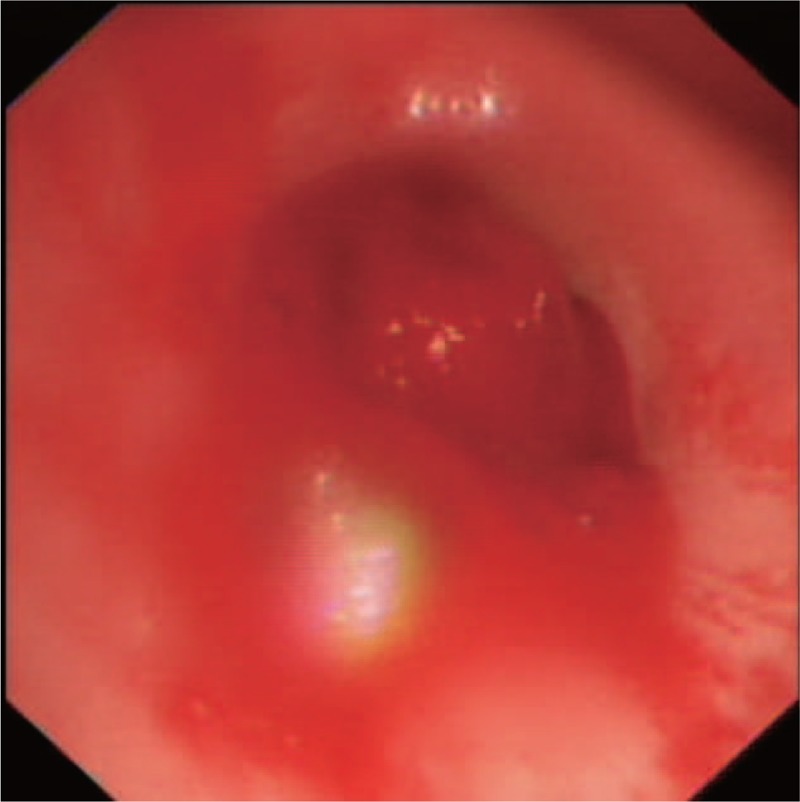
Interventions: She underwent a bronchoscopic examination, which revealed a mass blocking most of the upper endoluminal trachea. Thus, the mass was resected at the upper tracheal segment, followed by electrotome and argon plasma coagulation treatment. She was then transferred to the Thyroid Surgery Department. Thyroid surgeons took the surgical type of bilateral subtotal thyroidectomy + exploration of bilateral recurrent laryngeal nerve + dissection of the lymph node in neck central area + circumferential sleeve resection + end-to-end anastomosis + tracheotomy in the patient.
Outcomes: After surgery, she recovered well without any local recurrence or distant metastasis.
Lessons: When patients with PTC have haemoptysis, hoarseness, dyspnea, or any other symptoms, and the imaging examinations reveal a space-occupying lesion in the thyroid and airway, clinicians should focus on PTC with tracheal invasion, a bronchoscopic examination must be immediately performed because the subsequent surgical management depends on the degree of tracheal invasion.
Conflict of interest statement
The authors declare that there is no conflicts of interest.
Figures

Similar articles
-
Papillary thyroid carcinoma with invasion of the trachea.Ann Med Surg (Lond). 2024 Jun 4;86(8):4820-4824. doi: 10.1097/MS9.0000000000002233. eCollection 2024 Aug. Ann Med Surg (Lond). 2024. PMID: 39118773 Free PMC article.
-
Massive hemoptysis: an unusual presentation of papillary thyroid carcinoma due to tracheal invasion.BMJ Case Rep. 2019 Aug 21;12(8):e229330. doi: 10.1136/bcr-2019-229330. BMJ Case Rep. 2019. PMID: 31439567 Free PMC article.
-
Robot-assisted Sistrunk's operation, total thyroidectomy, and neck dissection via a transaxillary and retroauricular (TARA) approach in papillary carcinoma arising in thyroglossal duct cyst and thyroid gland.Ann Surg Oncol. 2012 Dec;19(13):4259-61. doi: 10.1245/s10434-012-2674-y. Epub 2012 Oct 16. Ann Surg Oncol. 2012. PMID: 23070784
-
Thyroid Carcinoma Showing Thymus-Like Differentiation (CASTLE) with Tracheal Invasion: A Case Report.Am J Case Rep. 2019 Dec 10;20:1845-1851. doi: 10.12659/AJCR.919208. Am J Case Rep. 2019. PMID: 31819030 Free PMC article. Review.
-
Metastatic papillary thyroid carcinoma with internal jugular vein tumor thrombus - A case report and review of the literature.Front Endocrinol (Lausanne). 2025 Jan 29;16:1505800. doi: 10.3389/fendo.2025.1505800. eCollection 2025. Front Endocrinol (Lausanne). 2025. PMID: 39944204 Free PMC article. Review.
Cited by
-
Management of papillary thyroid cancer with tracheal invasion and lung cancer: A case report.Oncol Lett. 2023 Feb 2;25(3):104. doi: 10.3892/ol.2023.13689. eCollection 2023 Mar. Oncol Lett. 2023. PMID: 36817043 Free PMC article.
-
Prognostic Indicators and Comparative Treatment Outcomes in High-Risk Thyroid Cancer with Laryngotracheal Invasion.Endocrinol Metab (Seoul). 2025 Apr;40(2):201-215. doi: 10.3803/EnM.2024.2033. Epub 2025 Jan 22. Endocrinol Metab (Seoul). 2025. PMID: 39838779 Free PMC article.
-
Papillary thyroid carcinoma with invasion of the trachea.Ann Med Surg (Lond). 2024 Jun 4;86(8):4820-4824. doi: 10.1097/MS9.0000000000002233. eCollection 2024 Aug. Ann Med Surg (Lond). 2024. PMID: 39118773 Free PMC article.
-
Transcription Factor E2F1 Exacerbates Papillary Thyroid Carcinoma Cell Growth and Invasion via Upregulation of LINC00152.Anal Cell Pathol (Amst). 2022 May 10;2022:7081611. doi: 10.1155/2022/7081611. eCollection 2022. Anal Cell Pathol (Amst). 2022. PMID: 35592867 Free PMC article.
-
The Current Understanding of the Molecular Pathogenesis of Papillary Thyroid Cancer.Int J Mol Sci. 2025 May 13;26(10):4646. doi: 10.3390/ijms26104646. Int J Mol Sci. 2025. PMID: 40429790 Free PMC article. Review.
References
-
- McCaffrey TV, Lipton RJ. Thyroid carcinoma invading the upper aerodigestive system. Laryngoscope 1990;100:824–30. - PubMed
-
- Cody HS, 3rd, Shah JP. Locally invasive, well-differentiated thyroid cancer. 22 years’ experience at Memorial Sloan-Kettering Cancer Center. Am J Surg 1981;142:480–3. - PubMed
-
- Djalilian M, Beahrs OH, Devine KD, et al. Intraluminal involvement of the larynx and trachea by thyroid cancer. Am J Surg 1974;128:500–4. - PubMed
-
- Sobin LH, Wittekind Ch<Eds>. TNM Classification of Malignant Tumours. New York: Wiley-Liss, Inc; 2002.
-
- Ortiz S, Rodríguez JM, Soria T, et al. Extrathyroid spread in papillary carcinoma of the thyroid: clinicopathological and prognostic study. Otolaryngol Head Neck Surg 2001;124:261–5. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
