

High-resolution computed tomography of the lung in patients with rheumatoid arthritis: Prevalence of interstitial lung disease involvement and determinants of abnormalities
- PMID: 31567944
- PMCID: PMC6756733
- DOI: 10.1097/MD.0000000000017088
High-resolution computed tomography of the lung in patients with rheumatoid arthritis: Prevalence of interstitial lung disease involvement and determinants of abnormalities
Abstract
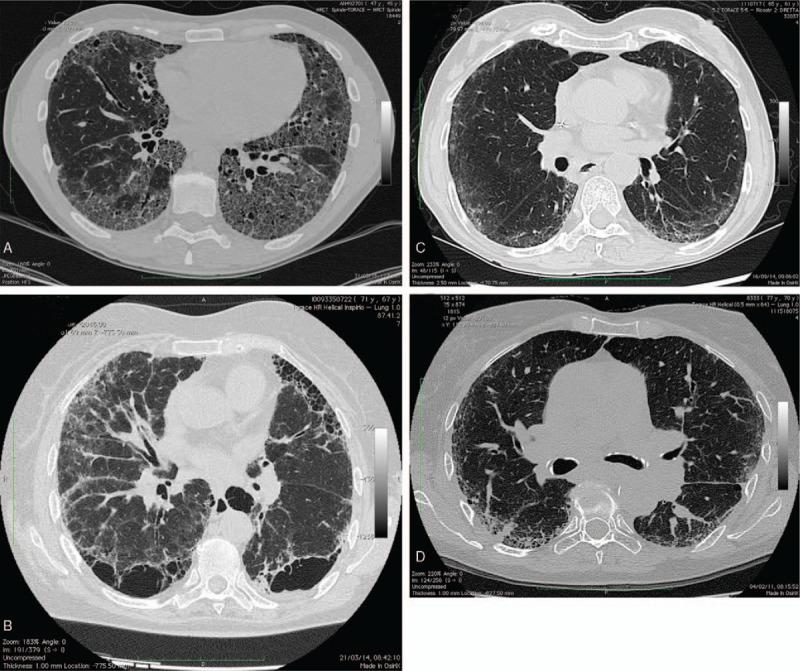
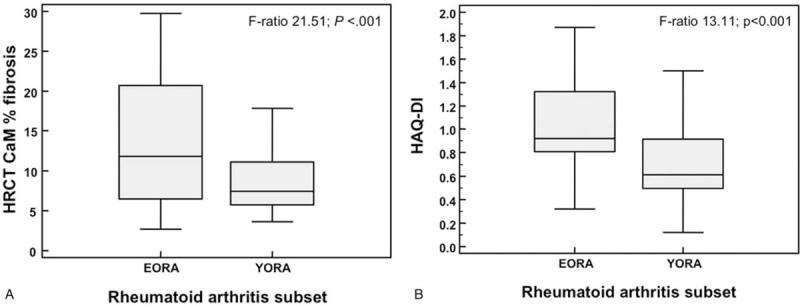
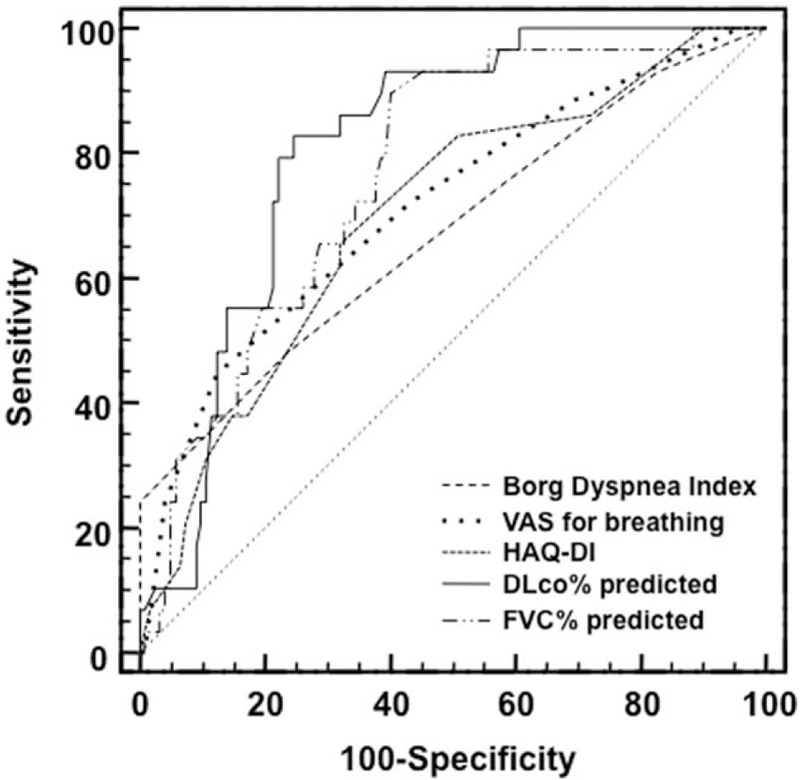
An international consensus for rheumatoid arthritis (RA) patients at risk of developing interstitial lung disease (ILD) is still lacking. The aims of study were to evaluate: the prevalence of ILD involvement in RA over high-resolution computed tomography (HRCT); the relationships between pulmonary function tests (PFTs), patient-centered measurements, and ILD; and the potential risk factors contributing to RA-ILD patients.Data regarding the clinical characteristics (age, sex, age at onset of RA), laboratory findings (rheumatoid factor [RF] and anti-citrullinated protein antibodies [ACPA]), respiratory functional assessment (forced vital capacity [FVC] and carbon monoxide diffusion capacity [DLCO]), patient-centred measures of dyspnea (PCMD), Health Assessment Questionnaire-Disability Index (HAQ-DI), and HRCT have collected retrospectively. HRCT abnormalities were evaluated using a conventional visual reader-based score (CoVR) and a computer-aided method (CaM). The relationships between the 2 HRCT scores-PFTs and PCMD-were calculated using Pearson correlation. The area under the receiving-operating characteristic (AUC-ROC) curve was calculated to determine the discriminatory performance of measurements between patients with and without ILD. The multivariate regression model was used to evaluate the association force between ILD and RA characteristics.In all, 151 patients (45 males and 106 females, mean age 53.4 ± 7.6 years) were included. ILD had been detected in 29 patients out of 151 (19.2%). Usual interstitial pneumonia was the most common HRCT. RA-ILD patients were older, and older at RA onset (both P < .01), with a higher HAQ-DI (P < .05) than patients without ILD. ACPA positivity and titer were higher in the RA-ILD group (P = .02). Extent and severity of ILD, and total CoVR and CaM score closely related to DLCO and PCMD (both P < .0001). A reduced DLCO was the most sensitive test for predicting the presence of ILD on HRCT (AUC-ROC 0.811 ± 0.037). Advanced age (P < .0001), age at RA onset (P = .025), ACPA titer (P = .004), and smoking (P = .008) were independent explanatory variables of HRCT damage in multivariate analysis.The RA-ILD is associated with age and older age of RA onset, smoking, and ACPA titer. DLCO seems to be the most sensitive parameter to predict ILD on HRCT, followed by PCMD.
Figures
References
-
- Salaffi F, De Angelis R, Grassi W. MArche Pain Prevalence; INvestigation Group (MAPPING) study. Prevalence of musculoskeletal conditions in an Italian population sample: results of a regional community-based study. I. The MAPPING study. Clin Exp Rheumatol 2005;23:819–28. - PubMed
-
- Carotti M, Salaffi F, Manganelli P, et al. The subclinical involvement of the lung in rheumatoid arthritis: evaluation by high-resolution computed tomography. Reumatismo 2001;53:280–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
