

Unilateral live twin tubal ectopic pregnancy presenting at 12 weeks of gestation: A case report
- PMID: 31567985
- PMCID: PMC6756681
- DOI: 10.1097/MD.0000000000017229
Unilateral live twin tubal ectopic pregnancy presenting at 12 weeks of gestation: A case report
Abstract
Rationale: Abdominal pain in pregnancy represents a demanding diagnostic challenge in the emergency department (ED) due to the extensive list of differential diagnoses to be considered, coupled with the possibility of each disease having nonclassical, atypical signs and symptoms, resultant from the patient's pregnant state. Additionally, emergency physicians (EPs) face limitations on investigative imaging modalities because of the need to minimize fetal radiation exposure. EPs have to tackle this diagnostic challenge while performing a balancing act to maximize both maternal and fetal outcomes in a time-sensitive manner, becauser any delays in decision-making at the ED may threaten the safety of mother and child. Two common causes of abdominal pain in pregnancy presenting to the ED are acute appendicitis and ectopic pregnancy. The latter is almost always diagnosed by 10 weeks of gestation. Here, we report an extremely rare case of unilateral live spontaneous twin tubal ectopic pregnancy presenting past 12 weeks of gestation, diagnosed after magnetic resonance imaging (MRI) of the abdomen.
Patient concerns: A 37-year-old gravida 2 para 1 at 12 weeks and 6 days of gestation presented to our ED with a 2-day history of right iliac fossa pain, not associated with vaginal bleeding, fever, diarrhea, and vomiting. On examination, she was tachycardic (pulse rate 124 beats/min) and hypertensive (blood pressure 142/88 mm Hg). There was marked tenderness and guarding at the lower abdomen.
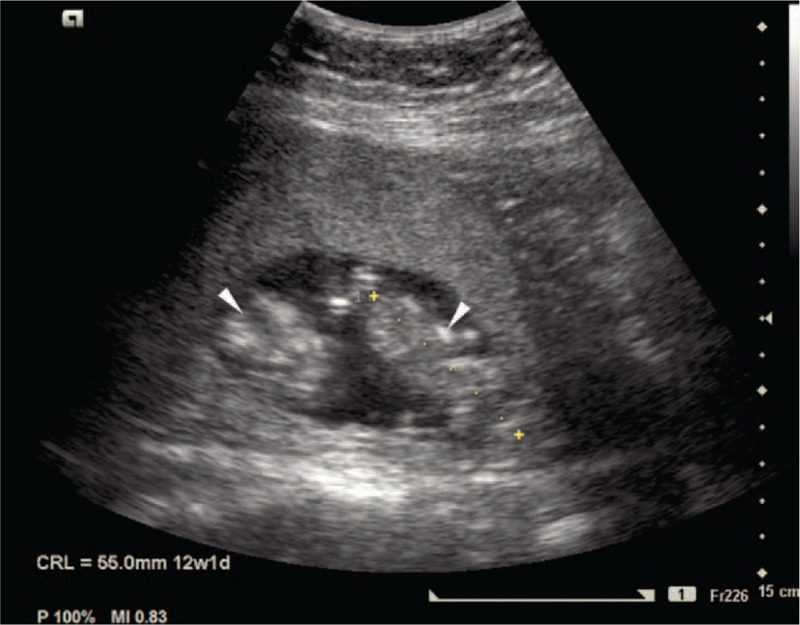
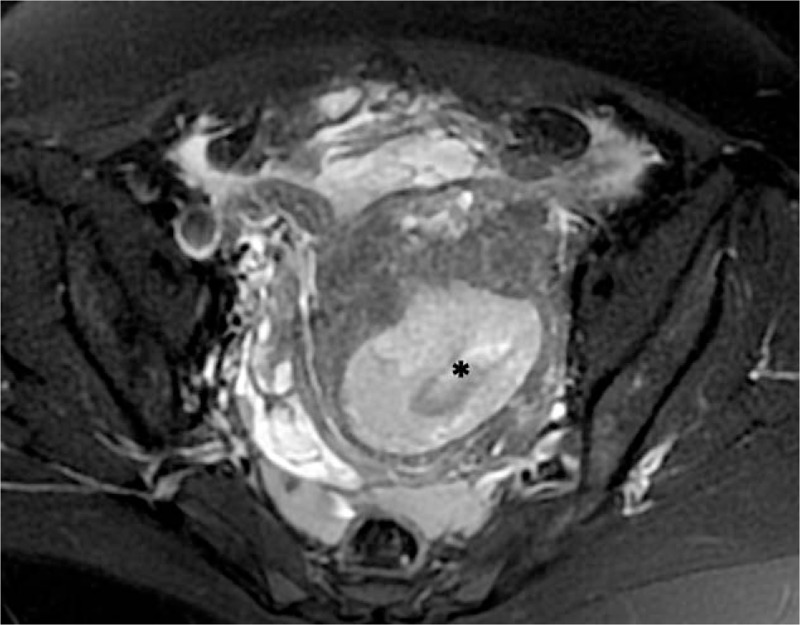
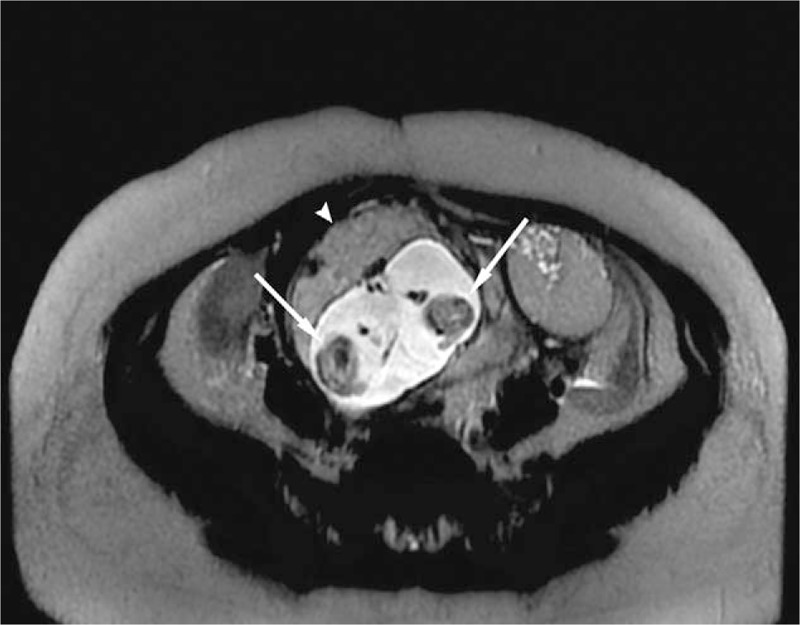
Diagnoses: Blood investigations were unremarkable, while abdominal ultrasonography found a live twin gestation with foetal heartbeats of 185 and 180 beats/min. MRI of the abdomen revealed an empty uterine cavity; 2 amniotic sacs and fetuses of diameter 10 cm, and a single placenta were noted in the right uterine adnexa. The patient was diagnosed with right live monochorionic diamniotic twin tubal pregnancy.
Intervention: Our patient underwent emergency laparoscopic right salpingectomy.
Outcomes: The operation was successful and her postoperative care remained uneventful up to discharge.
Lessons: Ectopic pregnancy cannot be ruled out based on prior normal antenatal examinations and gestational age of >10 weeks. EPs should not hesitate to order MRI scans for further evaluation if ultrasonography and laboratory findings are equivocal.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Misdiagnosis of appendicitis in tubally sterilized women.Aust N Z J Surg. 1993 Jan;63(1):68-70. doi: 10.1111/j.1445-2197.1993.tb00037.x. Aust N Z J Surg. 1993. PMID: 8466465 Review.
-
Exophytic interstitial ectopic pregnancy removal: novel use of Endoloop for uterine cavity preservation.Fertil Steril. 2023 Feb;119(2):336-338. doi: 10.1016/j.fertnstert.2022.10.019. Epub 2022 Nov 18. Fertil Steril. 2023. PMID: 36404156
-
Tubo-Ovarian ectopic pregnancy: A rare twin ectopic pregnancy.J Pak Med Assoc. 2024 Jun;74(6):1172-1174. doi: 10.47391/JPMA.9355. J Pak Med Assoc. 2024. PMID: 38948993
-
Tubal ectopic twin pregnancy of complete hydatidiform mole and coexisting embryo: A rare case report.Medicine (Baltimore). 2023 Jun 2;102(22):e33922. doi: 10.1097/MD.0000000000033922. Medicine (Baltimore). 2023. PMID: 37266634 Free PMC article.
-
Heterotopic triplet pregnancy (twin tubal) in a natural cycle with tubal rupture: case report and review of the literature.J Obstet Gynaecol Res. 2008 Aug;34(4 Pt 2):759-62. doi: 10.1111/j.1447-0756.2008.00921.x. J Obstet Gynaecol Res. 2008. PMID: 18840198 Review.
Cited by
-
Management of a spontaneously conceived live unilateral twin ectopic pregnancy in Australia: A case report.Case Rep Womens Health. 2021 Feb 12;30:e00300. doi: 10.1016/j.crwh.2021.e00300. eCollection 2021 Apr. Case Rep Womens Health. 2021. PMID: 33665142 Free PMC article.
-
Sonographically Positive Fetal Heartbeat in Unilateral Tubal Twin Pregnancy as a Rare Case With Literature Review.Cureus. 2023 May 30;15(5):e39697. doi: 10.7759/cureus.39697. eCollection 2023 May. Cureus. 2023. PMID: 37398746 Free PMC article.
-
Rare Unilateral Twin Ectopic Pregnancy After Frozen Embryo Transfer: A Case Report and Literature Review.Int Med Case Rep J. 2023 Nov 13;16:731-737. doi: 10.2147/IMCRJ.S409492. eCollection 2023. Int Med Case Rep J. 2023. PMID: 38020575 Free PMC article.
-
Unilateral Twin Ectopic Pregnancy: A Case Report from the Eastern Part of Ethiopia, Harar.Int Med Case Rep J. 2022 Sep 19;15:521-527. doi: 10.2147/IMCRJ.S382708. eCollection 2022. Int Med Case Rep J. 2022. PMID: 36157570 Free PMC article.
References
-
- Cappell MS, Friedel D. Abdominal pain during pregnancy. Gastroenterol Clin North Am 2003;32:1–58. - PubMed
-
- El-Amin Ali M, Yahia Al-Shehri M, Zaki ZM, et al. Acute abdomen in pregnancy. Int J Gynaecol Obstet 1998;62:31–6. - PubMed
-
- Tamir IL, Bongard FS, Klein SR. Acute appendicitis in the pregnant patient. Am J Surg 1990;160:571–5. discussion 575-576. - PubMed
-
- Alkatout I, Honemeyer U, Strauss A, et al. Clinical diagnosis and treatment of ectopic pregnancy. Obstet Gynecol Surv 2013;68:571–81. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
