

Hip Fractures: Therapy, Timing, and Complication Spectrum
- PMID: 31568676
- PMCID: PMC6904609
- DOI: 10.1111/os.12524
Hip Fractures: Therapy, Timing, and Complication Spectrum
Abstract
Objective: Investigation of the treatment of femur fractures and the type of femur fracture-associated complications regarding timing of surgery and length of hospital stay.
Methods: In this retrospective cohort study, a total of 358 hip fractures were evaluated retrospectively from 1 January 2008 until 31 December 2010 at a level I trauma center in Germany. Inclusion criteria was age >18 years and a proximal femur fracture. Both sexes were evaluated. Mean age was 75.5 years, most patients were female (63.7%). Intervention was the operative treatment of proximal femur fracture. Outcome parameters were time until surgery, complications, reoperations, mortality, and length of hospital stay.
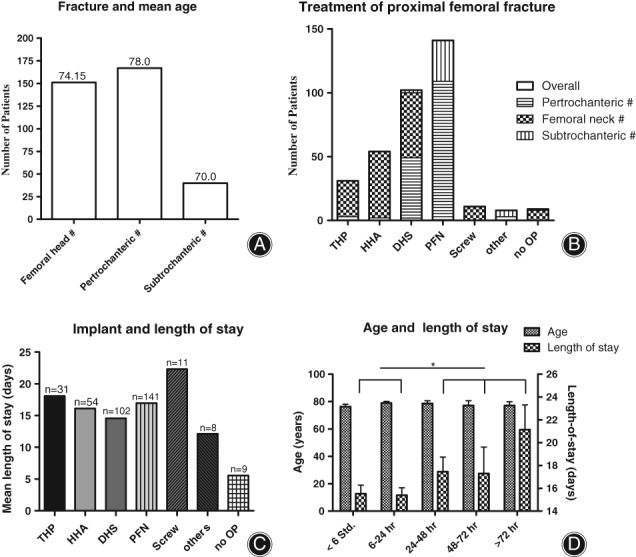
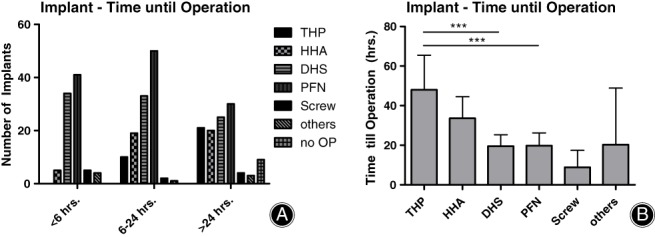
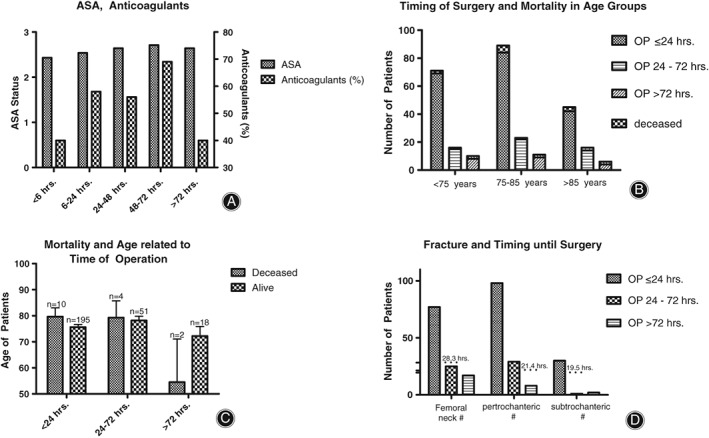
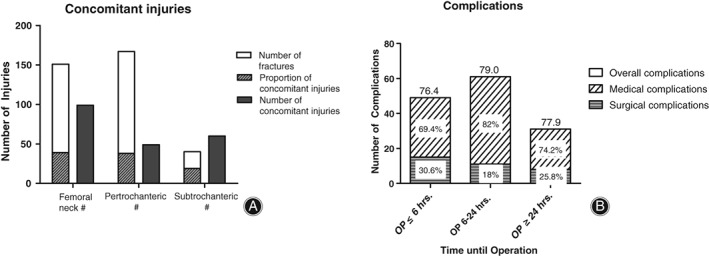
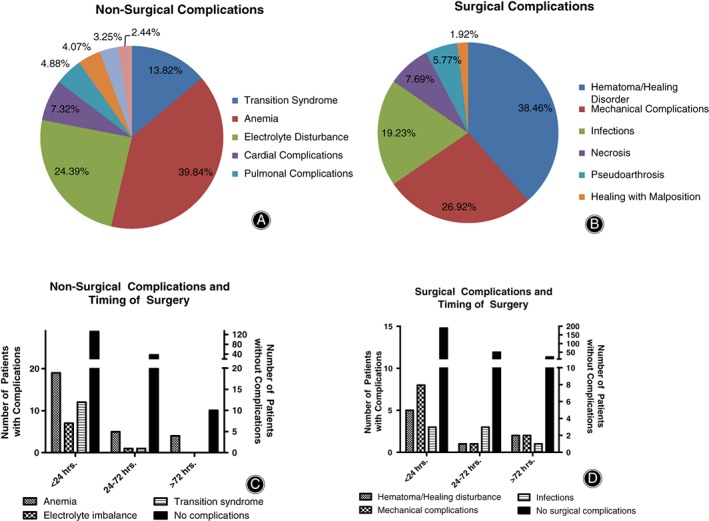
Results: Among the proximal femur fractures (n = 358), 46.6% were pertrochanteric, 11.2% subtrochanteric, and 42.2% femoral neck fractures. Operation upon hip fractures was managed regularly within 24 hours of injury (73%; mean for femoral neck: 28.3 hrs.; mean for pertrochanteric fractures: 21.4 hrs.; mean for subtrochanteric fractures: 19.5 hrs.). Delayed treatment, as well as implantation of hip total endoprosthesis (TEP), increased the overall length of hospital stay (15.4 vs 17.6 days; 18.1 vs 15.8 days). Accordingly, surgical procedures performed within 24 hours of injury resulted in a shorter hospital residence. Longest delay of operation was measured for hip fractures (28.3 hrs.). In 351 patients, secondary injuries were detected in 94 individuals (26%), with fractures being the most common secondary injury (n = 40). We recorded postoperative complications of nonsurgical and surgical origin, and 33.6% of our patient cohort displayed complications. Complications were distributed among 118 patients. There was no significant difference in complications regarding the time of operation, with most nonsurgical and surgical complications appearing within 24 hours after operation (n = 110 vs n = 31). Nonsurgical complications, such as anemia (n = 49) and electrolyte imbalances (n = 30), were observed more frequently than surgical complications (n = 107 vs n = 34); however, these complications were reduced by delay in surgery (82.0% in 6-24 hrs. vs 74.2% in ≥24 hrs.). Anticoagulant therapy and age did not affect postoperative complications. The hospital mortality of patients was 6.2%. Follow-up was restrained to ambulatory visits in the clinic.
Conclusions: Surgical management of hip fractures performed within 24 hours of injury minimizes hospital stay. We did not detect significant differences in the spectrum or number of complications regarding delay of surgery. Surgical complications mainly occur with rapid primary care, and medical complications can be reduced by more intensive preparation of patient and operation procedures.
Keywords: Age traumatology; Complications; Femoral neck fractures; Hip fractures; Pertrochanteric fracture.
© 2019 The Authors. Orthopaedic Surgery published by Chinese Orthopaedic Association and John Wiley & Sons Australia, Ltd.
Figures
References
-
- Böhm K, Tesch‐Römer C, Ziese T, eds. Gesundheit und Krankheit im Alter. Berlin: Robert Koch‐Inst, 2009.
-
- Hoffmann F, Glaeske G. Incidence of hip fracture in Germany‐‐person‐related analysis of health insurance population. Gesundheitswesen, 2006, 68: 161–164. - PubMed
-
- Minne HW, Pfeifer M, Wittenberg R, Würtz R. Schenkelhalsfrakturen in Deutschland: Prävention, Therapie, Inzidenz und sozioökonomische Bedeutung. Dtsch Arztebl, 2001, 98: 1751.
-
- Beck A, Rüter A. Therapiekonzepte bei Schenkelhalsfrakturen. Teil 1. Der Chirurg, 2000, 71: 240–248. - PubMed
-
- Icks A, Haastert B, Wildner M, Becker C, Meyer G. Trend of hip fracture incidence in Germany 1995‐2004: a population‐based study. Osteoporos Int, 2008, 19: 1139–1145. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
