

Prevention of Early Postoperative Decline: A Randomized, Controlled Feasibility Trial of Perioperative Cognitive Training
- PMID: 31569161
- PMCID: PMC7154961
- DOI: 10.1213/ANE.0000000000004469
Prevention of Early Postoperative Decline: A Randomized, Controlled Feasibility Trial of Perioperative Cognitive Training
Abstract
Background: Postoperative delirium and postoperative cognitive dysfunction (POCD) are common after cardiac surgery and contribute to an increased risk of postoperative complications, longer length of stay, and increased hospital mortality. Cognitive training (CT) may be able to durably improve cognitive reserve in areas deficient in delirium and POCD and, therefore, may potentially reduce the risk of these conditions. We sought to determine the feasibility and potential efficacy of a perioperative CT program to reduce the incidence of postoperative delirium and POCD in older cardiac surgery patients.
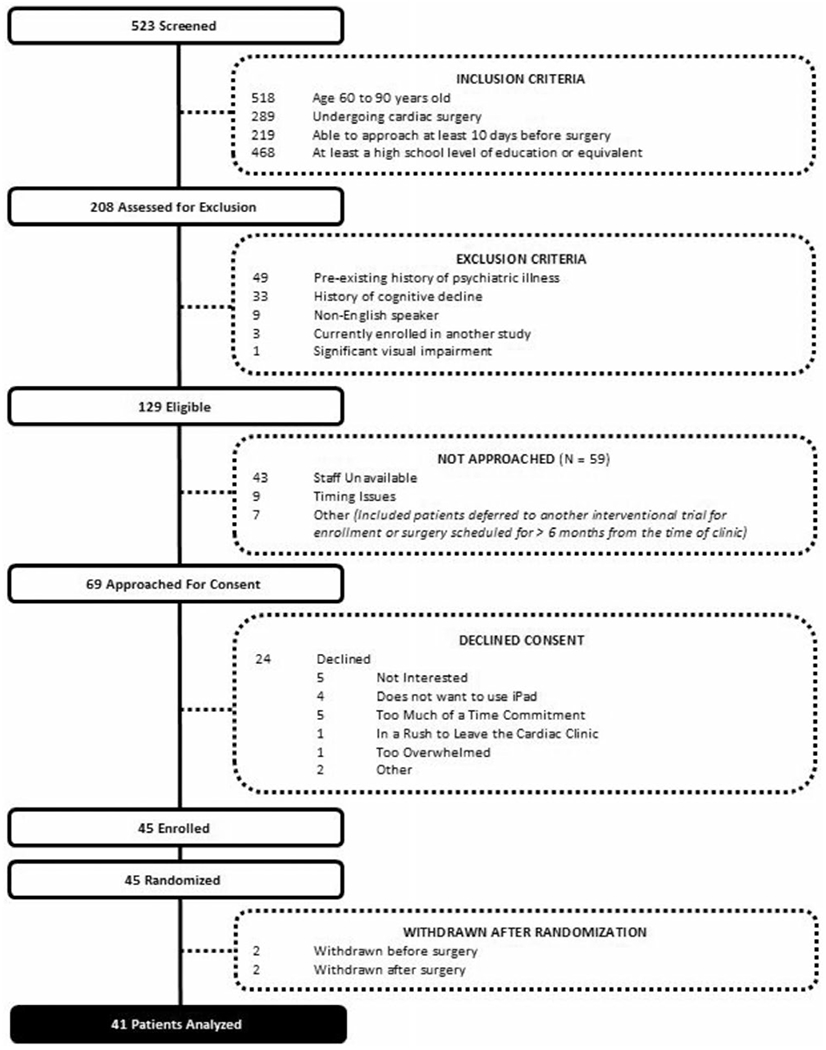
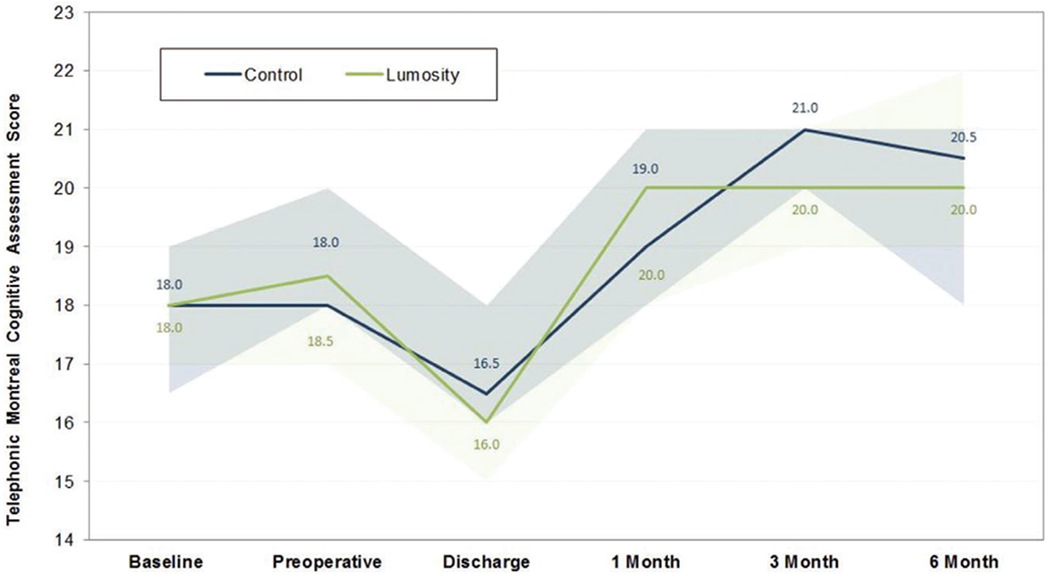
Methods: Randomized controlled trial at a single tertiary care center. Participants included 45 older adults age 60-90 undergoing cardiac surgery at least 10 days from enrollment. Participants were randomly assigned in a 1:1 fashion to either perioperative CT via a mobile device or a usual care control. The primary outcome of feasibility was evaluated by enrollment patterns and adherence to protocol. Secondary outcomes of postoperative delirium and POCD were assessed using the Confusion Assessment Method and the Montreal Cognitive Assessment, respectively. Patient satisfaction was assessed via a postoperative survey.
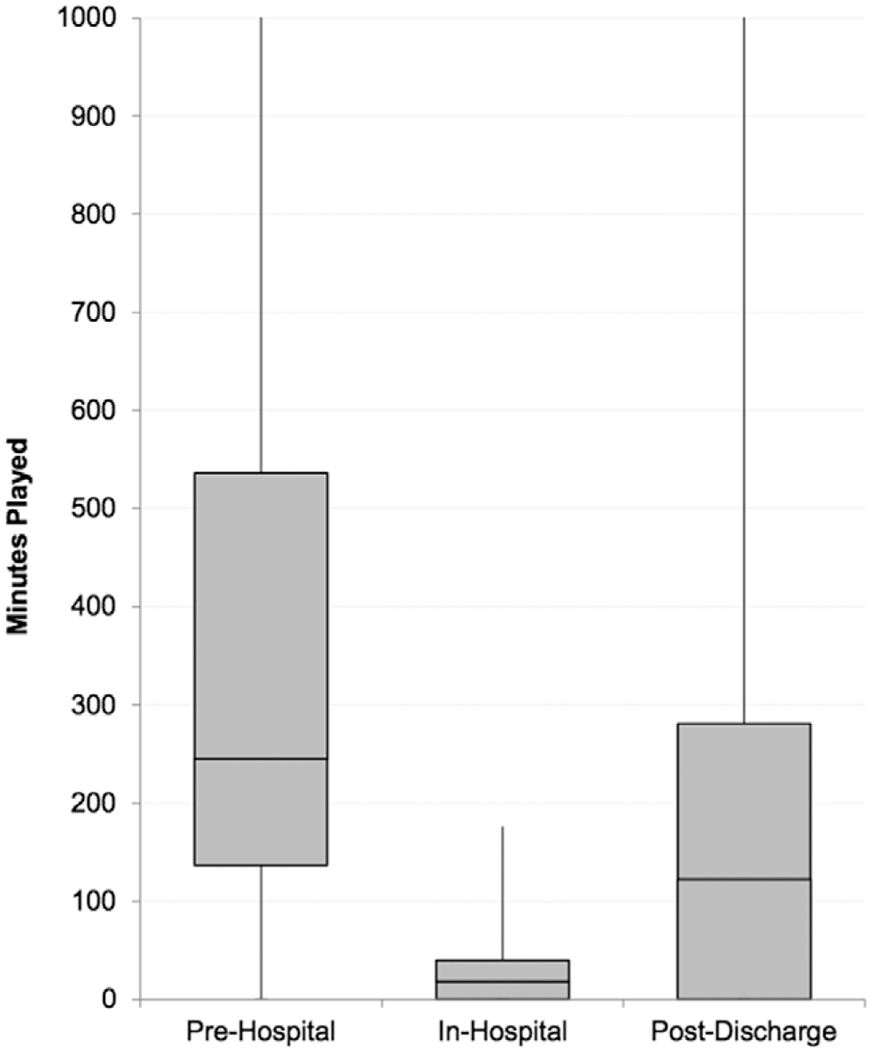
Results: Sixty-five percent of eligible patients were enrolled. Median (interquartile range [IQR]) adherence (as a percentage of prescribed minutes played) was 39% (20%-68%), 6% (0%-37%), and 19% (0%-56%) for the preoperative, immediate postoperative, and postdischarge periods, respectively. Median (IQR) training times were 245 (136-536), 18 (0-40), and 122 (0-281) minutes for each period, respectively. The incidence of postoperative delirium (CT group 5/20 [25%] versus control 3/20 [15%]; P = .69) and POCD (CT group 53% versus control 37%; P = .33) was not significantly different between groups for either outcome in this limited sample. CT participants reported a high level of agreement (on a scale of 0-100) with statements that the program was easy to use (median [IQR], 87 [75-97]) and enjoyable (85 [79-91]). CT participants agreed significantly more than controls that their memory (median [IQR], 75 [54-82] vs 51 [49-54]; P = .01) and thinking ability (median [IQR], 78 [64-83] vs 50 [41-68]; P = .01) improved as a result of their participation in the study.
Conclusions: A CT program designed for use in the preoperative period is an attractive target for future investigations of cognitive prehabilitation in older cardiac surgery patients. Changes in the functionality of the program and enrichment techniques may improve adherence in future trials. Further investigation is necessary to determine the potential efficacy of cognitive prehabilitation to reduce the risk of postoperative delirium and POCD.
Conflict of interest statement
DISCLOSURES
Figures
Comment in
-
Can Cognitive Training Improve Perioperative Brain Health?Anesth Analg. 2020 Mar;130(3):583-585. doi: 10.1213/ANE.0000000000004543. Anesth Analg. 2020. PMID: 32068586 Free PMC article. No abstract available.
-
Is a Trial of Perioperative Cognitive Training to Prevent Early Postoperative Cognitive Decline Actually Feasible?Anesth Analg. 2020 Aug;131(2):e75-e77. doi: 10.1213/ANE.0000000000004859. Anesth Analg. 2020. PMID: 33031670 No abstract available.
-
In Response.Anesth Analg. 2020 Aug;131(2):e77-e78. doi: 10.1213/ANE.0000000000004860. Anesth Analg. 2020. PMID: 33031671 No abstract available.
References
-
- Newman MF, Kirchner JL, Phillips-Bute B, et al. Longitudinal assessment of neurocognitive function after coronary-artery bypass surgery. N Engl J Med. 2001;344:395–402. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
