

Pathological transition as the arising mechanism for drug resistance in lung cancer
- PMID: 31570104
- PMCID: PMC6771104
- DOI: 10.1186/s40880-019-0402-8
Pathological transition as the arising mechanism for drug resistance in lung cancer
Abstract
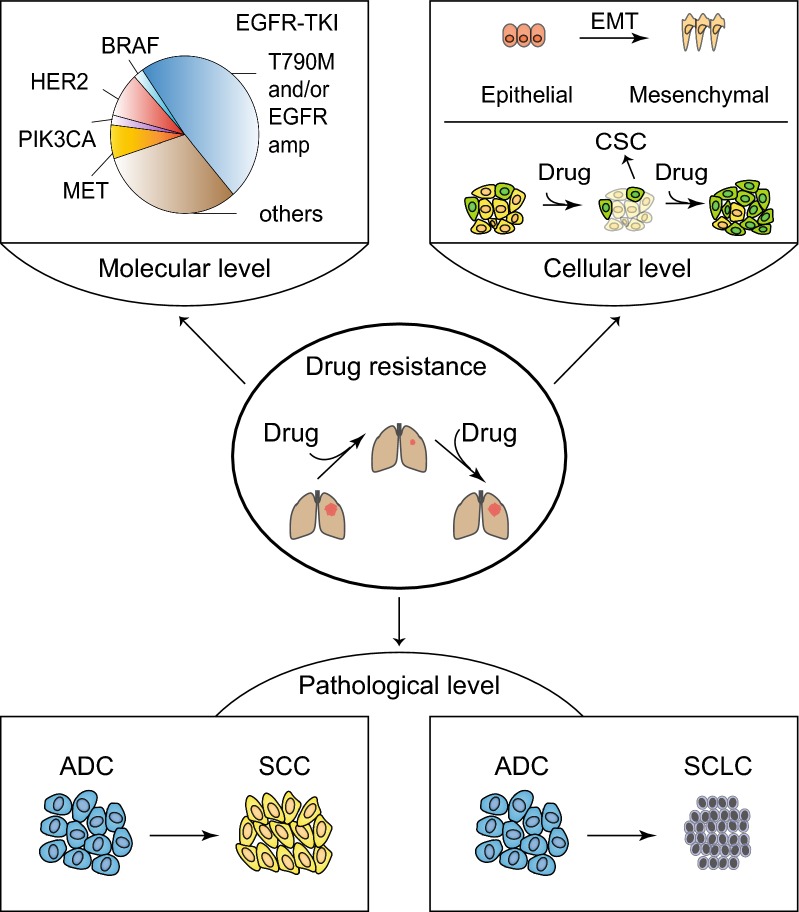
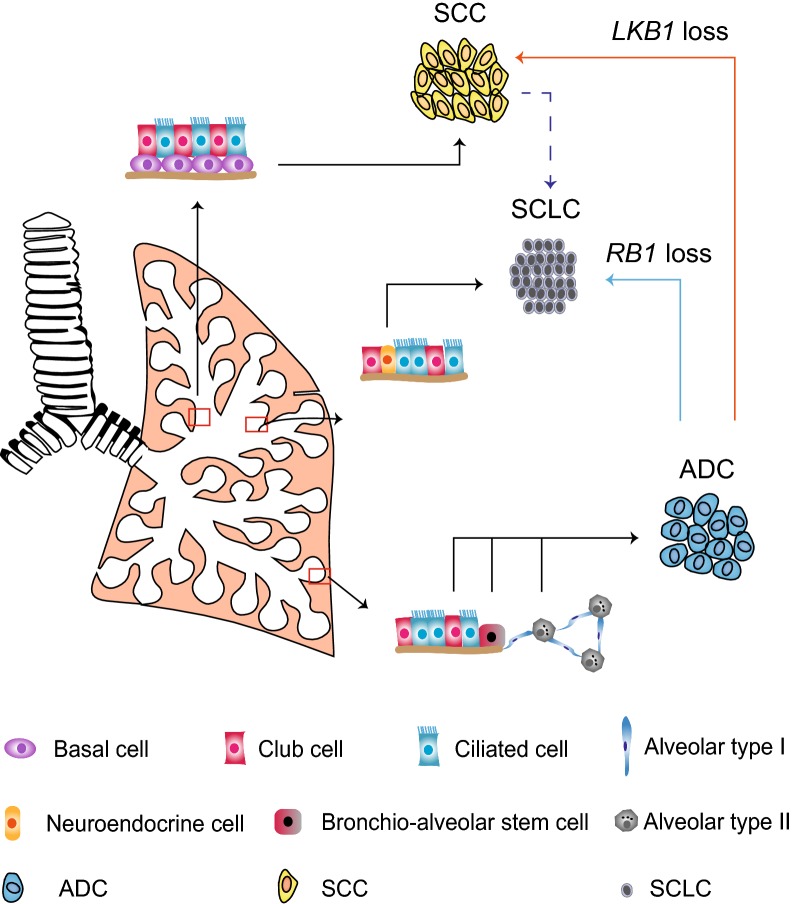
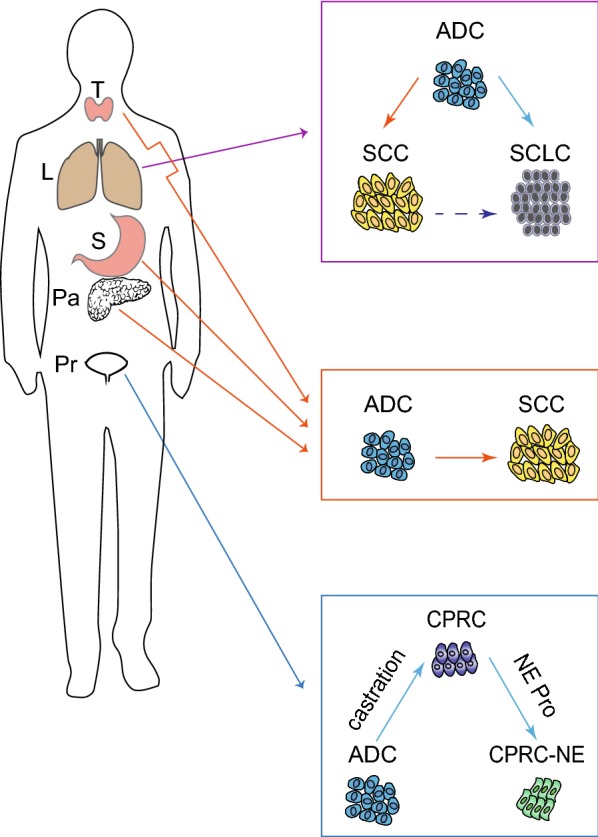
Despite the tremendous efforts for improving therapeutics of lung cancer patients, its prognosis remains disappointing. This can be largely attributed to the lack of comprehensive understanding of drug resistance leading to insufficient development of effective therapeutics in clinic. Based on the current progresses of lung cancer research, we classify drug resistance mechanisms into three different levels: molecular, cellular and pathological level. All these three levels have significantly contributed to the acquisition and evolution of drug resistance in clinic. Our understanding on drug resistance mechanisms has begun to change the way of clinical practice and improve patient prognosis. In this review, we focus on discussing the pathological changes linking to drug resistance as this has been largely overlooked in the past decades.
Keywords: Drug resistance; Lung cancer; Pathological transition.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Fujii T, Dracheva T, Player A, Chacko S, Clifford R, Strausberg RL, et al. A preliminary transcriptome map of non-small cell lung cancer. Can Res. 2002;62(12):3340. - PubMed
-
- Rekhtman N, Ang DC, Sima CS, Travis WD, Moreira AL. Immunohistochemical algorithm for differentiation of lung adenocarcinoma and squamous cell carcinoma based on large series of whole-tissue sections with validation in small specimens. Mod Pathol. 2011;24:1348. doi: 10.1038/modpathol.2011.92. - DOI - PubMed
-
- Righi L, Graziano P, Fornari A, Rossi G, Barbareschi M, Cavazza A, et al. Immunohistochemical subtyping of nonsmall cell lung cancer not otherwise specified in fine-needle aspiration cytology: a retrospective study of 103 cases with surgical correlation. Cancer. 2011;117(15):3416–3423. doi: 10.1002/cncr.25830. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
