

A population-specific material model for sagittal craniosynostosis to predict surgical shape outcomes
- PMID: 31571084
- PMCID: PMC7424404
- DOI: 10.1007/s10237-019-01229-y
A population-specific material model for sagittal craniosynostosis to predict surgical shape outcomes
Abstract
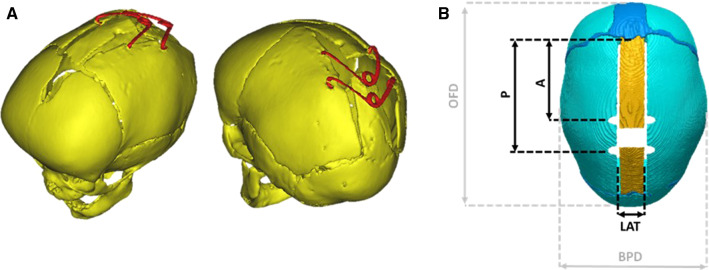
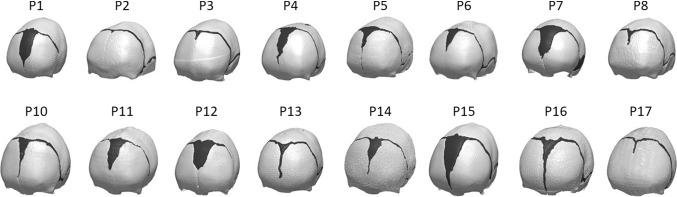
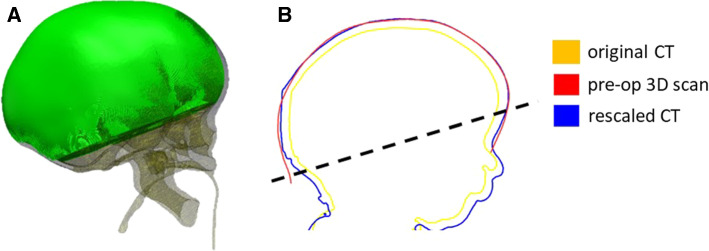
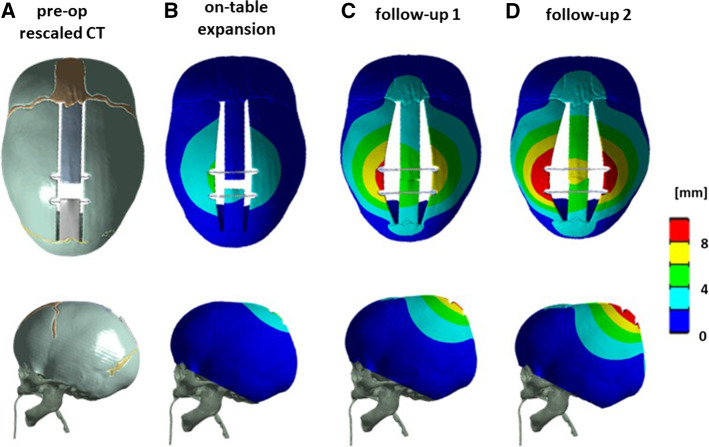
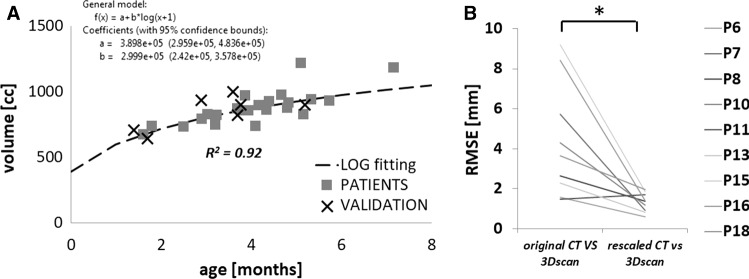
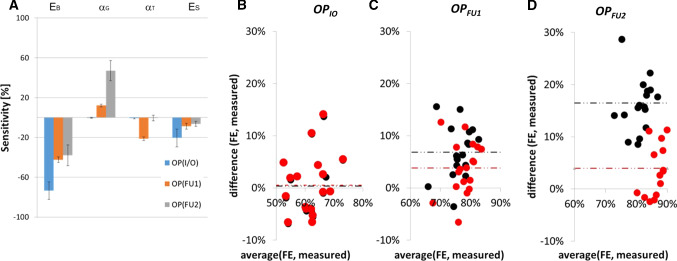
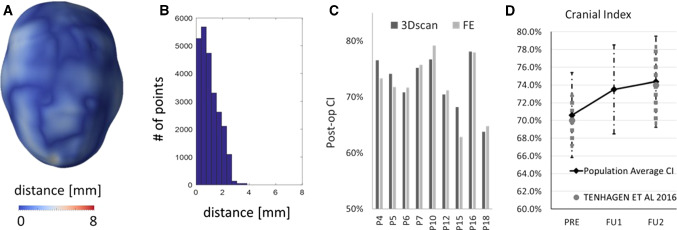
Sagittal craniosynostosis consists of premature fusion (ossification) of the sagittal suture during infancy, resulting in head deformity and brain growth restriction. Spring-assisted cranioplasty (SAC) entails skull incisions to free the fused suture and insertion of two springs (metallic distractors) to promote cranial reshaping. Although safe and effective, SAC outcomes remain uncertain. We aimed hereby to obtain and validate a skull material model for SAC outcome prediction. Computed tomography data relative to 18 patients were processed to simulate surgical cuts and spring location. A rescaling model for age matching was created using retrospective data and validated. Design of experiments was used to assess the effect of different material property parameters on the model output. Subsequent material optimization-using retrospective clinical spring measurements-was performed for nine patients. A population-derived material model was obtained and applied to the whole population. Results showed that bone Young's modulus and relaxation modulus had the largest effect on the model predictions: the use of the population-derived material model had a negligible effect on improving the prediction of on-table opening while significantly improved the prediction of spring kinematics at follow-up. The model was validated using on-table 3D scans for nine patients: the predicted head shape approximated within 2 mm the 3D scan model in 80% of the surface points, in 8 out of 9 patients. The accuracy and reliability of the developed computational model of SAC were increased using population data: this tool is now ready for prospective clinical application.
Keywords: Craniofacial surgery; Design of experiments; Finite element modelling; Scaphocephaly; Spring cranioplasty.
Figures
References
-
- ANSYS 17.2. User Manual
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
