

Efficacy and Safety of a Fixed Combination of Cinnarizine 20 mg and Dimenhydrinate 40 mg vs Betahistine Dihydrochloride 16 mg in Patients with Peripheral Vestibular Vertigo: A Prospective, Multinational, Multicenter, Double-Blind, Randomized, Non-inferiority Clinical Trial
- PMID: 31571128
- PMCID: PMC6800407
- DOI: 10.1007/s40261-019-00858-6
Efficacy and Safety of a Fixed Combination of Cinnarizine 20 mg and Dimenhydrinate 40 mg vs Betahistine Dihydrochloride 16 mg in Patients with Peripheral Vestibular Vertigo: A Prospective, Multinational, Multicenter, Double-Blind, Randomized, Non-inferiority Clinical Trial
Abstract
Background and objective: Vertigo derived from peripheral vestibular disorders is quite frequently encountered in daily clinical practice and can be a severely disabling symptom associated with substantial impairment of health-related quality of life for the affected patients. Betahistine, a structural analogue of histamine and presumably the most widely prescribed anti-vertigo drug worldwide, has previously been shown to be an effective and safe treatment for these patients. The objective of the present study was to evaluate whether the fixed combination of cinnarizine and dimenhydrinate (Arlevert®) is non-inferior and thus a potentially useful alternative to betahistine dihydrochloride in the treatment of patients suffering from peripheral vestibular vertigo.
Methods: In this prospective, multicenter, double-blind, randomized, non-inferiority clinical trial, outpatients from 8 ENT clinics in Austria, Bulgaria, the Czech Republic and Russia were randomly assigned to receive three times daily one tablet of either the fixed combination cinnarizine 20 mg/dimenhydrinate 40 mg or betahistine dihydrochloride 16 mg for 4 weeks. Primary endpoint was the reduction of the mean vertigo score (MVS), a validated 12-item composite score defined as the mean of 6 vertigo symptoms (dystasia and walking unsteadiness, staggering, rotary sensation, tendency to fall, lift sensation, blackout) and 6 trigger factors for vertigo (change of position, bowing, getting up, driving by car/train, head movements, eye movement), after 4 weeks of therapy, as judged by the patient on a 5-point visual analogue scale (VAS). The non-inferiority margin was set to 0.3. Secondary outcomes included the patient's and investigator's judgment of global efficacy, the patient's rating of impairment of daily activities, and safety/tolerability of the treatments.
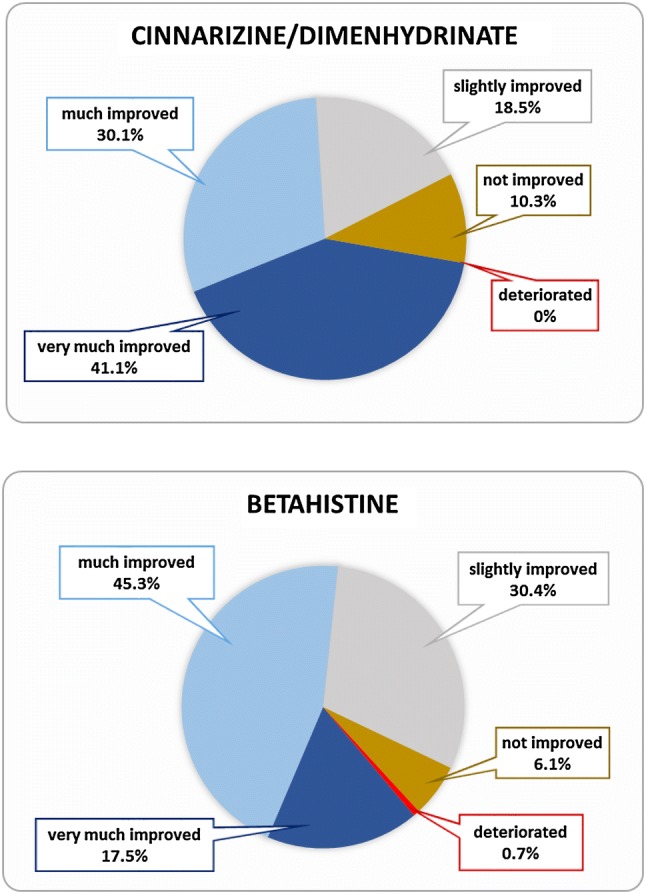
Results: Three hundred and six patients (mean age 53.5 years, approximately 60% female) were enrolled and randomized to the fixed combination cinnarizine/dimenhydrinate (n = 152) or betahistine (n = 154) groups; 297 patients completed the study and 294 (146 and 148, respectively) were valid for the per-protocol analysis, which was used for the non-inferiority analysis. Treatment with cinnarizine/dimenhydrinate led to a stronger reduction of the MVS [least squares mean (LSM)] after 4-week therapy (primary endpoint) in comparison to betahistine (0.395 vs 0.488; difference: - 0.093, 95% CI - 0.180; - 0.007, p = 0.035); since the upper limit of the two-sided 95% confidence interval was not only below the non-inferiority margin of 0.3, but also entirely below 0, superiority of the fixed combination could be demonstrated. The combination preparation was also more effective after 1 week of therapy and received more favorable patient's ratings on overall efficacy and impairment of daily activities. Both treatments were very well tolerated. Only 12 patients (3.92%) reported 13 non-serious adverse events; 2 cinnarizine/dimenhydrinate-treated patients discontinued the study prematurely due to adverse events as compared to 5 betahistine-treated patients.
Conclusion: The fixed combination of cinnarizine 20 mg and dimenhydrinate 40 mg was found to be not only non-inferior, but superior to betahistine 16 mg in the improvement of peripheral vestibular vertigo. Furthermore, taking into account a good and slightly favorable safety profile, the present study provides evidence that the fixed-combination preparation is a potent and even superior alternative to betahistine in the treatment of vertigo related to peripheral vestibular disorders.
Study registration: EudraCT No. 2011-004025-27.
Conflict of interest statement
Arne W. Scholtz, Ales Hahn, Bohdana Stefflova, Daniela Mezhidieva, Sergey V. Ryazantsev, Alexander Paschinin and Natalia Kunelskaya have no conflicts of interest that are directly relevant to the content of this article. Kai Schumacher is an employee of Berlin-Chemie AG/Menarini and Gerhard Weisshaar is an employee of Hennig Arzneimittel.
Figures



Comment in
-
The Challenges of Studying Peripheral Vestibular Vertigo.Clin Drug Investig. 2020 Jan;40(1):99-100. doi: 10.1007/s40261-019-00871-9. Clin Drug Investig. 2020. PMID: 31676932 No abstract available.
-
Authors' Reply to "The Challenges of Studying Peripheral Vestibular Vertigo".Clin Drug Investig. 2020 Jan;40(1):101-102. doi: 10.1007/s40261-019-00872-8. Clin Drug Investig. 2020. PMID: 31679119 No abstract available.
Similar articles
-
Efficacy and Safety of a Fixed-Dose Combination of Cinnarizine 20 mg and Dimenhydrinate 40 mg in the Treatment of Patients with Vestibular Vertigo: An Individual Patient Data Meta-Analysis of Randomised, Double-Blind, Controlled Clinical Trials.Clin Drug Investig. 2022 Sep;42(9):705-720. doi: 10.1007/s40261-022-01184-0. Epub 2022 Jul 21. Clin Drug Investig. 2022. PMID: 35864302 Free PMC article.
-
Comparison of the therapeutic efficacy of a fixed low-dose combination of cinnarizine and dimenhydrinate with betahistine in vestibular neuritis: a randomized, double-blind, non-inferiority study.Clin Drug Investig. 2012 Jun 1;32(6):387-99. doi: 10.2165/11632410-000000000-00000. Clin Drug Investig. 2012. PMID: 22506537 Clinical Trial.
-
Efficacy and tolerability of a fixed low-dose combination of cinnarizine and dimenhydrinate in the treatment of vertigo: a 4-week, randomized, double-blind, active- and placebo-controlled, parallel-group, outpatient study.Clin Ther. 2007 Jan;29(1):84-98. doi: 10.1016/j.clinthera.2007.01.010. Clin Ther. 2007. PMID: 17379049 Clinical Trial.
-
Association of cinnarizine and betahistine in prophylactic therapy for Ménière's disease with and without migraine.Acta Otorhinolaryngol Ital. 2014 Oct;34(5):349-53. Acta Otorhinolaryngol Ital. 2014. PMID: 25709150 Free PMC article. Review.
-
Use of betahistine in the treatment of peripheral vertigo.Acta Otolaryngol. 2015;135(12):1205-11. doi: 10.3109/00016489.2015.1072873. Epub 2015 Aug 6. Acta Otolaryngol. 2015. PMID: 26245698 Review.
Cited by
-
Histaminergic System and Vestibular Function in Normal and Pathological Conditions.Curr Neuropharmacol. 2024;22(11):1826-1845. doi: 10.2174/1570159X22666240319123151. Curr Neuropharmacol. 2024. PMID: 38504566 Free PMC article. Review.
-
Efficacy and Safety of a Fixed-Dose Combination of Cinnarizine 20 mg and Dimenhydrinate 40 mg in the Treatment of Patients with Vestibular Vertigo: An Individual Patient Data Meta-Analysis of Randomised, Double-Blind, Controlled Clinical Trials.Clin Drug Investig. 2022 Sep;42(9):705-720. doi: 10.1007/s40261-022-01184-0. Epub 2022 Jul 21. Clin Drug Investig. 2022. PMID: 35864302 Free PMC article.
-
Drug-Drug Interactions in Vestibular Diseases, Clinical Problems, and Medico-Legal Implications.Int J Environ Res Public Health. 2021 Dec 8;18(24):12936. doi: 10.3390/ijerph182412936. Int J Environ Res Public Health. 2021. PMID: 34948545 Free PMC article. Review.
-
Simultaneous estimation of dimenhydrinate, cinnarizine and their toxic impurities benzophenone and diphenylmethylpiperazine; in silico toxicity profiling of impurities.RSC Adv. 2020 Oct 9;10(61):37439-37448. doi: 10.1039/d0ra06147f. eCollection 2020 Oct 7. RSC Adv. 2020. PMID: 35521250 Free PMC article.
-
The Challenges of Studying Peripheral Vestibular Vertigo.Clin Drug Investig. 2020 Jan;40(1):99-100. doi: 10.1007/s40261-019-00871-9. Clin Drug Investig. 2020. PMID: 31676932 No abstract available.
References
-
- Brandt T, Dieterich M, Strupp M. Vertigo and dizziness—common complaints. 2. London: Springer; 2013.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
