

Preterm birth phenotypes in women with autoimmune rheumatic diseases: a population-based cohort study
- PMID: 31571337
- PMCID: PMC6908743
- DOI: 10.1111/1471-0528.15970
Preterm birth phenotypes in women with autoimmune rheumatic diseases: a population-based cohort study
Abstract
Objective: To investigate preterm birth (PTB) phenotypes in women with different autoimmune rheumatic diseases in a large population-based cohort.
Design: Retrospective cohort study.
Setting: California, USA.
Population: All live singleton births in California between 2007 and 2011 were analysed. Patients with autoimmune disease at delivery were identified by International Classification of Diseases, Ninth Revision , Clinical Modification (ICD-9-CM), codes for systemic lupus erythematosus (SLE), systemic sclerosis (SSc), rheumatoid arthritis (RA), polymyositis/dermatomyositis (DM/PM), and juvenile idiopathic arthritis (JIA).
Methods: Maternally linked hospital and birth certificate records of 2 481 516 deliveries were assessed (SLE n = 2272, RA n = 1501, SSc n = 88, JIA n = 187, DM/PM n = 38). Multivariable Poisson regression models estimated the risk ratios (RRs) for different PTB phenotypes (relative to term deliveries) for each autoimmune disease compared with the general obstetric population, adjusting for maternal age, race/ethnicity, body mass index, smoking, education, payer, parity, and prenatal care.
Main outcome measures: Preterm birth (PTB) was assessed overall (20-36 weeks of gestation) and by subphenotype: preterm prelabour rupture of membranes (PPROM), spontaneous birth, or medically indicated PTB. The risk of PTB overall and for each phenotype was partitioned by gestational age: early (20-31 weeks of gestation) and late (32-36 weeks of gestation).
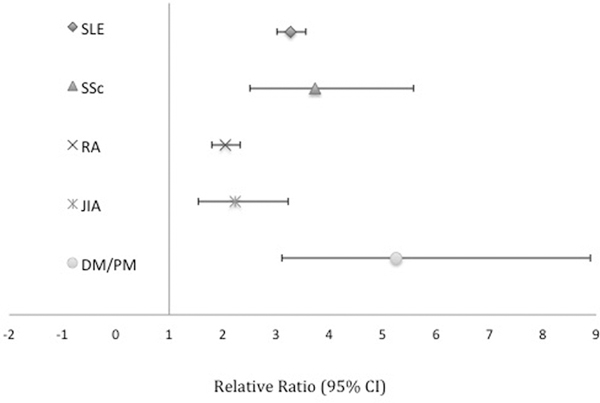
Results: Risks for PTB were elevated for each autoimmune disease evaluated: SLE (RR 3.27, 95% CI 3.01-3.56), RA (RR 2.04, 95% CI 1.79-2.33), SSc (RR 3.74, 95% CI 2.51-5.58), JIA (RR 2.23, 95% CI 1.54-3.23), and DM/PM (RR 5.26, 95% CI 3.12-8.89). These elevated risks were observed for the majority of PTB phenotypes as well.
Conclusions: Women with systemic autoimmune diseases appear to have an elevated risk of various PTB phenotypes. Therefore, preconception counselling and close monitoring during pregnancy is crucial.
Tweetable abstract: This study found that women with systemic autoimmune diseases have an elevated risk of preterm birth phenotypes.
Keywords: Autoimmune disease; connective tissue disease; eclampsia; pre-eclampsia; preterm birth; preterm prelabour rupture of membranes.
© 2019 Royal College of Obstetricians and Gynaecologists.
Conflict of interest statement
Disclosure of Interests:
The authors report no conflicts of interest. Completed disclosure of interest forms are available to view online as supporting information.
Figures
References
-
- Saigal S, Doyle LW. An overview of mortality and sequelae of preterm birth from infancy to adulthood. Lancet. 2008;371(9608):261–269. - PubMed
-
- Sibai BM. Diagnosis and management of gestational hypertension and preeclampsia. Obstet Gynecol. 2003;102(1):181–192. - PubMed
-
- Lisonkova S, Sabr Y, Mayer C, Young C, Skoll A, Joseph KS. Maternal morbidity associated with early-onset and late-onset preeclampsia. Obstet Gynecol. 2014;124(4):771–781. - PubMed
-
- Kurkinen-Raty M, Koivisto M, Jouppila P. Preterm delivery for maternal or fetal indications: maternal morbidity, neonatal outcome and late sequelae in infants. BJOG. 2000;107(5):648–655. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
