

Combined intravenous immunoglobulin and methylprednisolone as induction treatment in chronic inflammatory demyelinating polyneuropathy (OPTIC protocol): a prospective pilot study
- PMID: 31571349
- PMCID: PMC7028131
- DOI: 10.1111/ene.14096
Combined intravenous immunoglobulin and methylprednisolone as induction treatment in chronic inflammatory demyelinating polyneuropathy (OPTIC protocol): a prospective pilot study
Abstract
Background and purpose: We hypothesized that combining intravenous immunoglobulin (IVIg) and intravenous methylprednisolone (IVMP) leads to more frequent remission compared with IVIg alone while maintaining the fast efficacy of IVIg. In this uncontrolled pilot study, we evaluated remission, rate of improvement and safety in patients with chronic inflammatory demyelinating polyradiculoneuropathy receiving induction treatment with combined IVIg and IVMP.
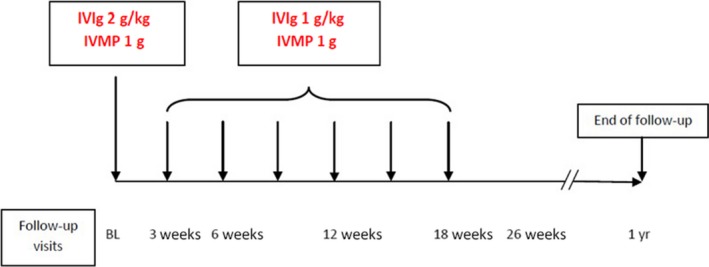
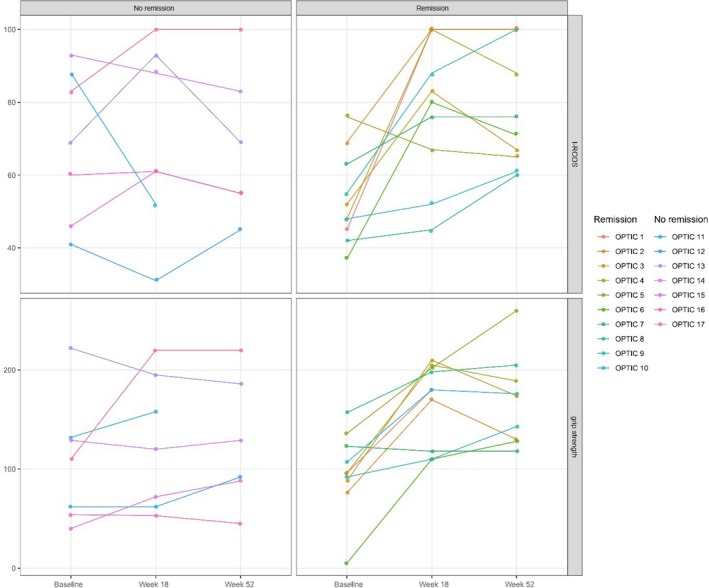
Methods: Consecutive treatment-naive patients with chronic inflammatory demyelinating polyradiculoneuropathy were treated with IVIg infusions, consisting of a 2 g/kg loading dose and 1 g/kg maintenance treatment every 3 weeks, combined with 3-weekly 1-g IVMP infusions, for a total of 18 weeks. The cumulative steroid dose was 7 g. Primary outcome was remission at 1 year in patients who completed the treatment schedule. Remission was defined as improvement at 18 weeks without the need for further immune treatment between end of the treatment schedule and 1-year follow-up. Improvement was defined as a minimal clinically important difference on the Inflammatory Rasch-Built Overall Disability Scale and/or an increase of ≥8 kPa in grip strength between baseline and week 18.
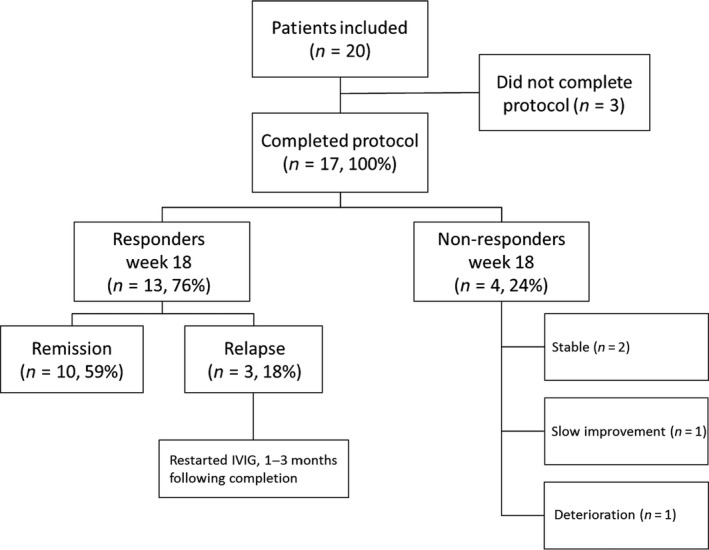
Results: A total of 20 patients were included; 17 completed the treatment schedule. A total of 13 (76%) of these patients improved at 18 weeks after start of treatment and 10 (59%) patients were in remission at 1 year. Serious adverse events were found in four patients.
Conclusions: Short-term combined induction treatment with IVIg and IVMP induced remission in almost 60% of patients who completed the treatment schedule. Combined induction therapy was generally well tolerated. A randomized controlled trial is currently running to confirm efficacy and safety of IVMP as add-on treatment to IVIg.
Keywords: chronic inflammatory demyelinating polyradiculoneuropathy; corticosteroids; intravenous immunoglobulin.
© 2019 The Authors. European Journal of Neurology published by John Wiley & Sons Ltd on behalf of European Academy of Neurology.
Conflict of interest statement
R. Hadden received personal and departmental payments from CSL Behring and Grifols. I.N. van Schaik reports departmental honoraria for serving on scientific advisory boards for CSL Behring and Baxter. He chaired a steering committee for CSL Behring. He is a member of the Scientific Board of the Kreuth III meeting. F. Eftimov reports grants from Prinses Beatrix Spierfonds, Netherlands Organization for Health Research and Development, and a consulting fee from CSL Behring, UCB Pharma and Aserta Pharma that was paid to the Institution, outside the submitted work. The other authors declare no financial or other conflicts of interest.
Figures
References
-
- van den Bergh PY, Hadden RD, Bouche P, et al European Federation of Neurological Societies/Peripheral Nerve Society guideline on management of CIDP: report of a joint task force of the EFNS/PNS – first revision. Eur J Neurol 2010; 17: 356–363. - PubMed
-
- Nobile‐Orazio E, Cocito D, Jann S, et al Intravenous immunoglobulin versus intravenous methylprednisolone for CIDP: a randomised controlled trial. Lancet Neurol 2012; 11: 493–502. - PubMed
-
- van Schaik IN, Eftimov F, van Doorn PA, et al Pulsed high‐dose dexamethasone versus standard prednisolone treatment for CIDP (PREDICT‐study): a double‐blind, randomised, controlled trial. Lancet Neurol 2010; 9: 245–253. - PubMed
-
- Latov N, Deng C, Dalakas MC, et al Timing and course of clinical response to intravenous immunoglobulin in CIDP. Arch Neurol 2010; 67: 802–807. - PubMed
-
- Eftimov F, Vermeulen M, van Doorn PA, Brusse E, van Schaik IN. Long‐term remission of CIDP after pulsed dexamethasone or short‐term prednisolone treatment. Neurology 2012; 78: 1079–1084. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
