

Macular edema associated with non-infectious uveitis: pathophysiology, etiology, prevalence, impact and management challenges
- PMID: 31571815
- PMCID: PMC6750710
- DOI: 10.2147/OPTH.S180580
Macular edema associated with non-infectious uveitis: pathophysiology, etiology, prevalence, impact and management challenges
Abstract
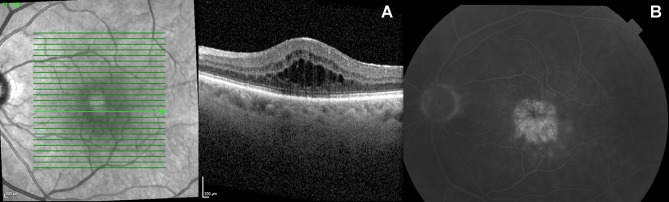
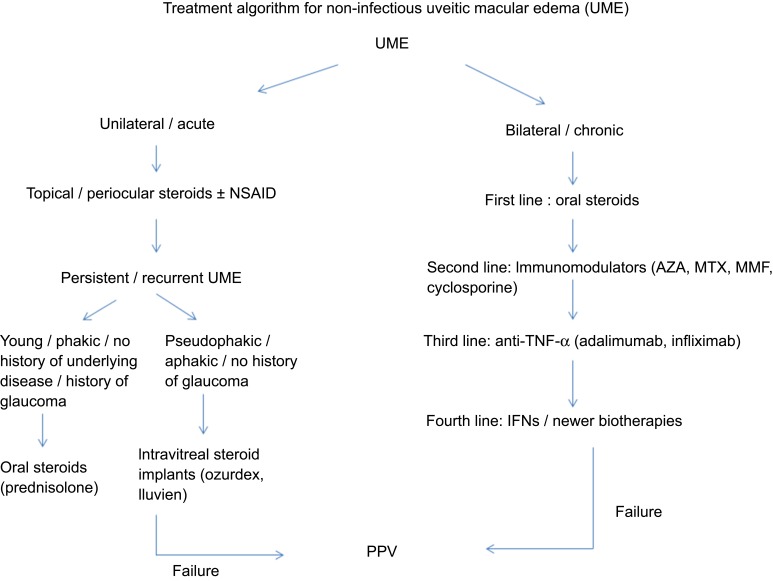
Macular edema (ME) is the most common sight-threatening complication in uveitis. The diagnostic and therapeutic management of the uveitic macular edema (UME) might be challenging due to the complex diagnostic workup and the difficulties physicians face to find the underlying cause, and due to its usually recurrent nature and the fact that it can be refractory to conventional treatment. Some of the mild cases can be treated with topical steroids, which can be combined with non-steroid anti-inflammatory drugs. However, immunomodulators such as methotrexate, tacrolimus, azathioprine, cyclosporine and mycophenolate mofetil together with anti-tumor necrosis factor-α (anti-TNF alpha) monoclonal antibodies such as adalimumab and infliximab, may be required to control the inflammation and the associated ME in refractory cases, or when an underlying disease is present. This review of the literature will focus mostly on the non-infectious UME.
Keywords: NSAIDs; anti-TNF alpha; corticosteroids; immunomodulators; macular edema; non-infectious uveitis.
© 2019 Massa et al.
Conflict of interest statement
The authors report no conflicts of interest in this work.
Figures

References
-
- Evans M. Uveitis In: Yanoff M, Duker J, editors. Ophthalmology. 4th ed. Philadelphia: Elsevier; 2014:687.
-
- Paivonsalo-Hietanen T, Tuominen J, Vaahtoranta-Lehtonen H, Saari KM. Incidence and prevalence of different uveitis entities in Finland. Acta Ophthalmol Scand. 1997;75(1):76–81. - PubMed
-
- Jabs DA, Nussenblatt RB, Rosenbaum JT, Standardization of Uveitis Nomenclature (SUN) Working Group. Standardization of uveitis nomenclature for reporting clinical data. Results of the First International Workshop. Am J Ophthalmol. 2005;140(3):509–516. doi: 10.1016/j.ajo.2005.03.057 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
