

Brivaracetam in the treatment of epilepsy: a review of clinical trial data
- PMID: 31571877
- PMCID: PMC6750854
- DOI: 10.2147/NDT.S143548
Brivaracetam in the treatment of epilepsy: a review of clinical trial data
Abstract
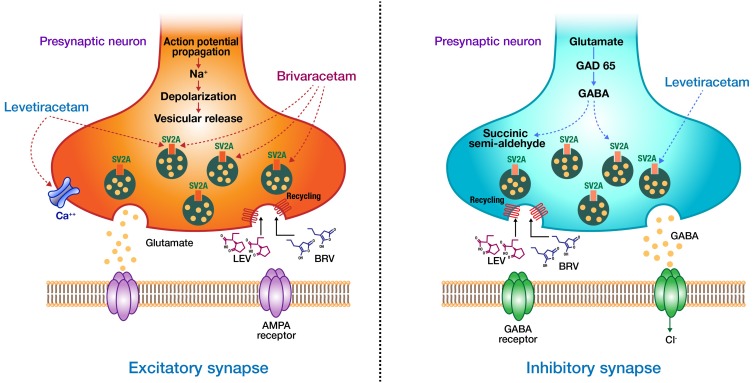
Brivaracetam (BRV), an analog of levetiracetam (LEV), was discovered during a target-based rational drug discovery program that aimed to identify potent synaptic vesicle protein 2A (SV2A) ligands. Among the 12,000 compounds screened in vitro, BRV was found to have 15-30 times greater affinity for SV2A and faster brain permeability than LEV. Although preclinical and post-marketing studies suggest broad spectrum of efficacy, BRV is currently only approved as monotherapy and adjunctive therapy of focal-onset seizures in patients age 4 years and older. This review examines the use of BRV as add-on (5-200 mg/day) therapy for epilepsy with a particular emphasis on the six regulatory randomized clinical trialsinvolving 2399 participants. Participants receiving BRV add-on at doses of 50-200 mg/day were more likely to experience a 50% or greater reduction in seizure frequency (pooled risk ratio [RR]) 1.79 with 95% CI of 1.51-2.12) than those receiving placebo. Participants receiving BRV were also more likely to attain seizure freedom (57 [3.3%] vs 4 [0.5%]; RR 4.74, 95% CI 2.00-11.25) than those receiving placebo. In addition, BRV demonstrated a favorable safety profile similar to placebo across all BRV doses. Treatment emergent adverse events significantly associated with BRV were irritability, fatigue, somnolence, and dizziness. Post-hoc analysis of regulatory trials, post-marketing studies, and indirect comparison meta-analyses demonstrated equivalent efficacy and better tolerability of BRV when compared to other antiseizure drugs. Further, these studies appear to suggest that behavioral adverse events are likely to be less frequent and less severe with BRV than LEV. Therefore, switching to BRV may be considered for patients who have seizure control with LEV, but who cannot tolerate its behavioral adverse effects. In this setting, immediate switch from LEV to BRV at a 10:1-15:1 ratio without titration is feasible. Further research is needed to examine the long-term tolerability and efficacy of BRV as well as its role in the treatment of other types of epilepsies, particularly dementia-related epilepsy and brain tumor-related epilepsy.
Keywords: antiepileptic drugs; brivaracetam; drug-resistant epilepsy; focal epilepsy; psychiatric adverse events; levetiracetam.
© 2019 Feyissa.
Conflict of interest statement
The author reports no conflicts of interest in this work.
Figures

Similar articles
-
Brivaracetam efficacy and safety in focal epilepsy.Expert Rev Neurother. 2019 Oct;19(10):955-964. doi: 10.1080/14737175.2019.1631160. Epub 2019 Jun 24. Expert Rev Neurother. 2019. PMID: 31195850 Review.
-
Narrative Review of Brivaracetam: Preclinical Profile and Clinical Benefits in the Treatment of Patients with Epilepsy.Adv Ther. 2024 Jul;41(7):2682-2699. doi: 10.1007/s12325-024-02876-z. Epub 2024 May 29. Adv Ther. 2024. PMID: 38811492 Free PMC article. Review.
-
Brivaracetam: Rationale for discovery and preclinical profile of a selective SV2A ligand for epilepsy treatment.Epilepsia. 2016 Apr;57(4):538-48. doi: 10.1111/epi.13340. Epub 2016 Feb 26. Epilepsia. 2016. PMID: 26920914 Review.
-
Adjunctive brivaracetam in adults with uncontrolled focal epilepsy: results from a double-blind, randomized, placebo-controlled trial.Epilepsia. 2014 Jan;55(1):47-56. doi: 10.1111/epi.12432. Epub 2013 Oct 28. Epilepsia. 2014. PMID: 24256083 Clinical Trial.
-
Brivaracetam as adjunctive treatment for uncontrolled partial epilepsy in adults: a phase III randomized, double-blind, placebo-controlled trial.Epilepsia. 2014 Jan;55(1):57-66. doi: 10.1111/epi.12433. Epub 2013 Nov 8. Epilepsia. 2014. PMID: 24446953 Clinical Trial.
Cited by
-
Development of SV2A Ligands for Epilepsy Treatment: A Review of Levetiracetam, Brivaracetam, and Padsevonil.Neurosci Bull. 2024 May;40(5):594-608. doi: 10.1007/s12264-023-01138-2. Epub 2023 Oct 28. Neurosci Bull. 2024. PMID: 37897555 Free PMC article. Review.
-
The Single-Dose Pharmacokinetics of a Compounded Levetiracetam Formulation and Bioequivalence to a Commercial Formulation in Healthy Dogs.J Vet Pharmacol Ther. 2025 Mar;48(2):67-75. doi: 10.1111/jvp.13490. Epub 2024 Nov 13. J Vet Pharmacol Ther. 2025. PMID: 39535310 Free PMC article.
-
The Integrated Effects of Brivaracetam, a Selective Analog of Levetiracetam, on Ionic Currents and Neuronal Excitability.Biomedicines. 2021 Apr 1;9(4):369. doi: 10.3390/biomedicines9040369. Biomedicines. 2021. PMID: 33916190 Free PMC article.
-
Investigating the Impact of Epilepsy on Cognitive Function: A Narrative Review.Cureus. 2023 Jun 30;15(6):e41223. doi: 10.7759/cureus.41223. eCollection 2023 Jun. Cureus. 2023. PMID: 37525802 Free PMC article. Review.
-
Functional genomics screens reveal a role for TBC1D24 and SV2B in antibody-dependent enhancement of dengue virus infection.J Virol. 2024 Nov 19;98(11):e0158224. doi: 10.1128/jvi.01582-24. Epub 2024 Oct 8. J Virol. 2024. PMID: 39377586 Free PMC article.
References
LinkOut - more resources
Full Text Sources
