

Management Strategies for POSEIDON Groups 3 and 4
- PMID: 31572298
- PMCID: PMC6749147
- DOI: 10.3389/fendo.2019.00614
Management Strategies for POSEIDON Groups 3 and 4
Abstract
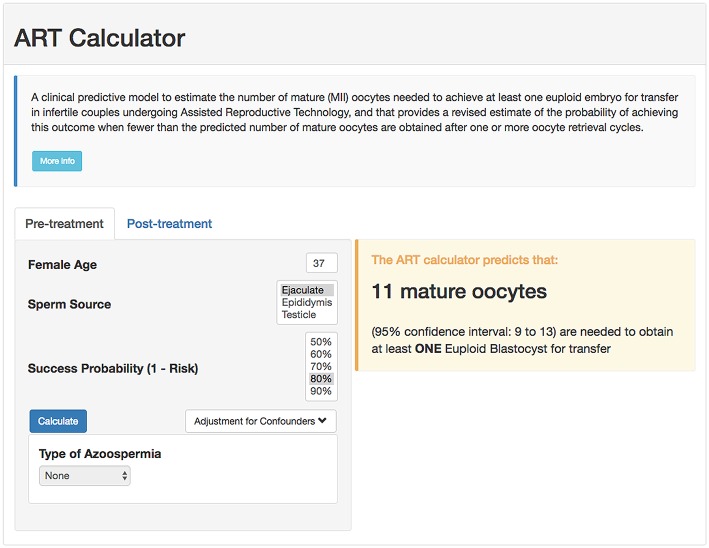
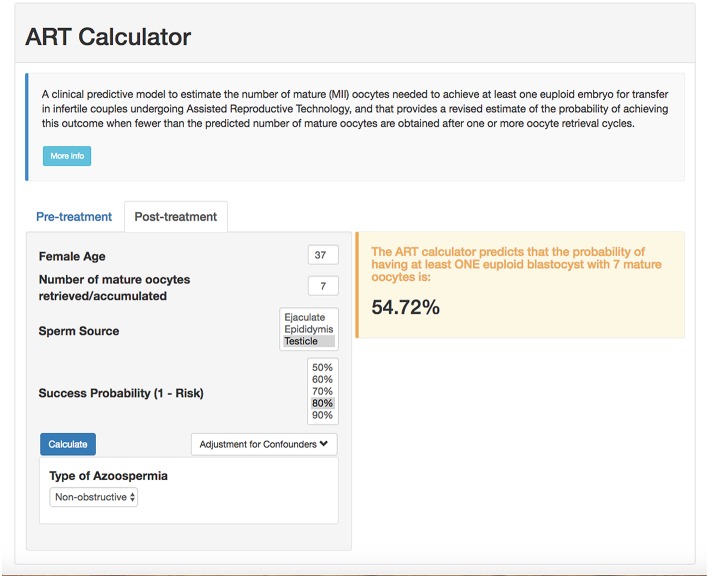
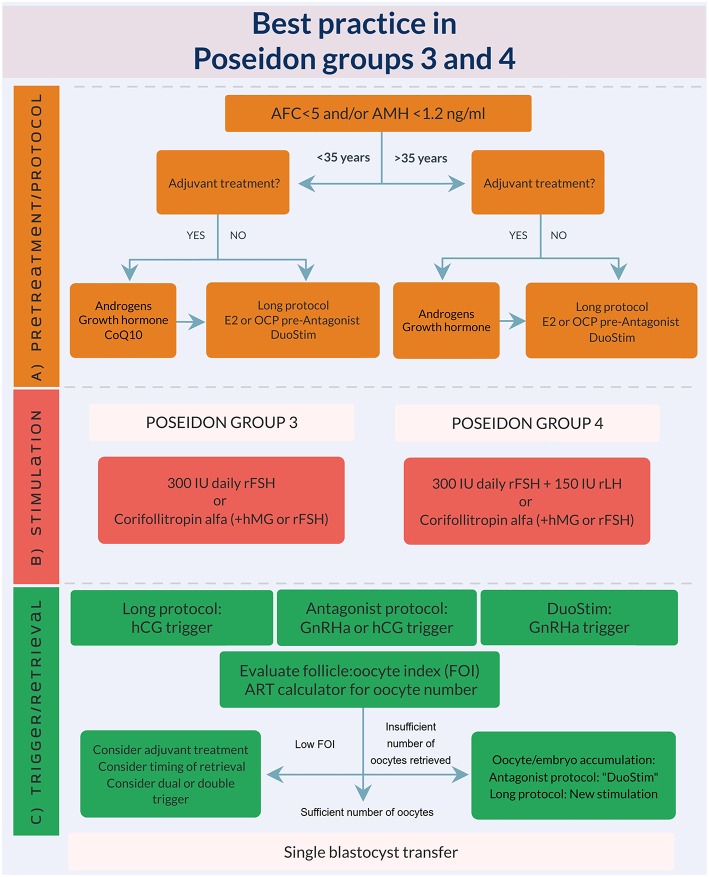
In the POSEIDON classification, patients belonging to groups 3 and 4 share the same common feature of a poor ovarian reserve which independently of age renders them at high risk of a poor reproductive outcome. Overall, POSEIDON groups 1-4 constitute approximately 47% of patients attending assisted reproductive technology (ART) treatment. With the increasing delay in childbearing, POSEIDON group 4 seems to increase in numbers now in some centers constituting more than 50% of the total POSEIDON population, whereas group 3 patients constitute approximately 10%. Both POSEIDON groups 3 and 4 patients require special attention as regards pre-treatment strategy, ovarian stimulation, adjuvant treatment, and ovulation trigger strategy in order to optimize the probability of having at least one euploid blastocyst for transfer. Although more evidence is needed, recent advances seem to have increased the reproductive outcomes in the poor prognosis patient. The key to success is individualization in all steps of ART treatment. Herein, we review the recent evidence for the management of POSEIDON groups 3 and 4.
Keywords: ART calculator; Bologna criteria; POSEIDON criteria; blastocyst; controlled ovarian stimulation; poor ovarian response; pregnancy.
Copyright © 2019 Haahr, Dosouto, Alviggi, Esteves and Humaidan.
Figures
Comment in
-
Commentary: Management Strategies for POSEIDON Groups 3 and 4.Front Endocrinol (Lausanne). 2020 Jan 24;10:920. doi: 10.3389/fendo.2019.00920. eCollection 2019. Front Endocrinol (Lausanne). 2020. PMID: 32038485 Free PMC article. No abstract available.
-
Commentary: Management Strategies for POSEIDON Groups 3 and 4.Front Endocrinol (Lausanne). 2020 Feb 4;11:34. doi: 10.3389/fendo.2020.00034. eCollection 2020. Front Endocrinol (Lausanne). 2020. PMID: 32117060 Free PMC article. No abstract available.
References
-
- Poseidon Group (Patient-Oriented Strategies Encompassing IndividualizeD Oocyte Number) Alviggi C, Andersen CY, Buehler K, Conforti A, De Placido G, et al. A new more detailed stratification of low responders to ovarian stimulation: from a poor ovarian response to a low prognosis concept. Fertil Steril. (2016) 105:1452–3. 10.1016/j.fertnstert.2016.02.005 - DOI - PubMed
-
- Alviggi C, Conforti A, Esteves SC, Vallone R, Venturella R, Staiano S, et al. Understanding ovarian hypo-response to exogenous gonadotropin in ovarian stimulation and its new proposed marker-the Follicle-To-Oocyte (FOI) index. Front Endocrinol. (2018) 9:589. 10.3389/fendo.2018.00589 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources