

Sequelae of Fetal Infection in a Non-human Primate Model of Listeriosis
- PMID: 31572310
- PMCID: PMC6749046
- DOI: 10.3389/fmicb.2019.02021
Sequelae of Fetal Infection in a Non-human Primate Model of Listeriosis
Abstract
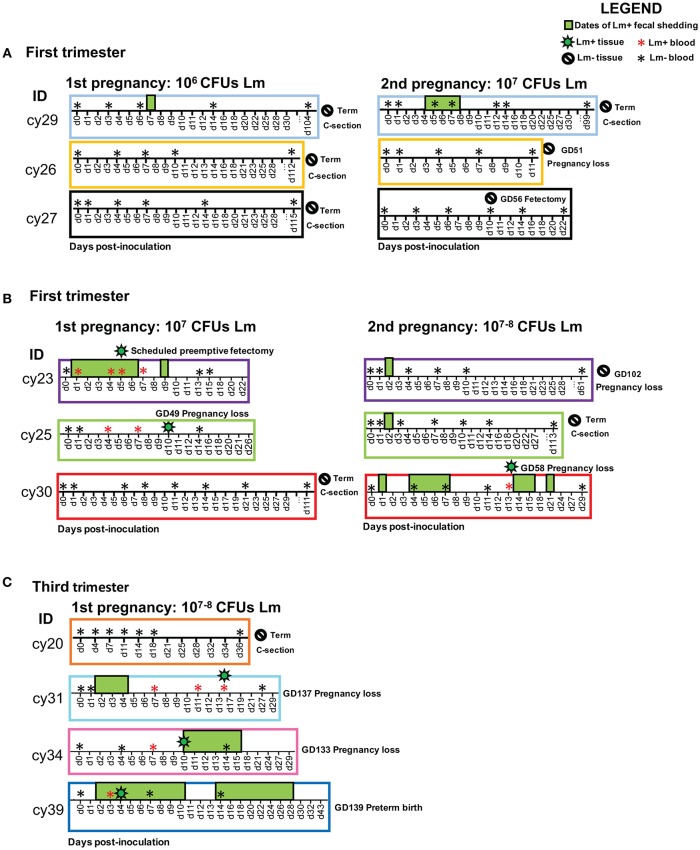
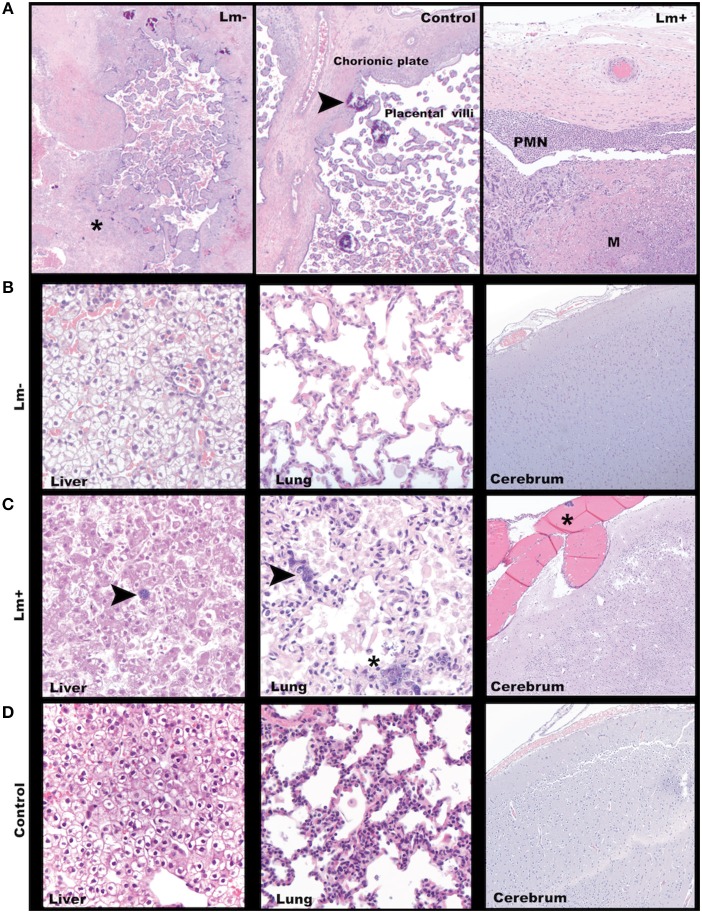
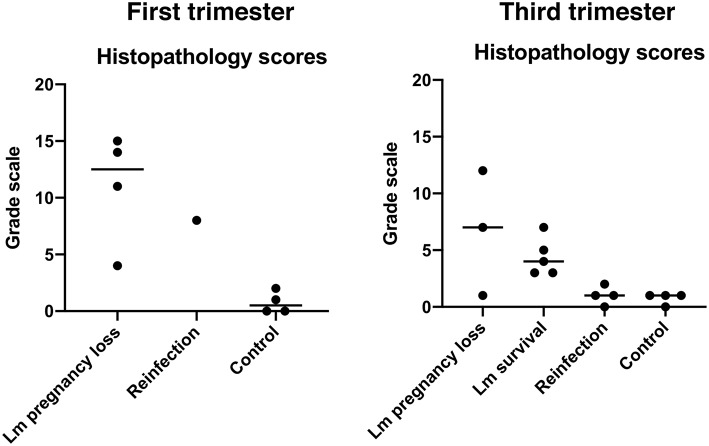
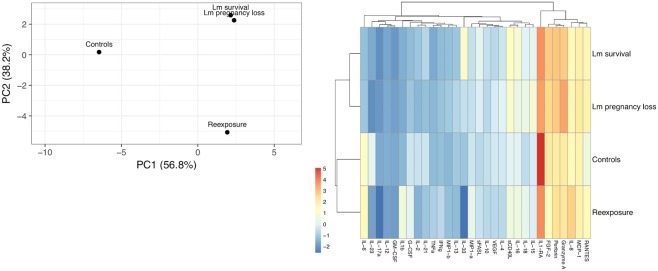
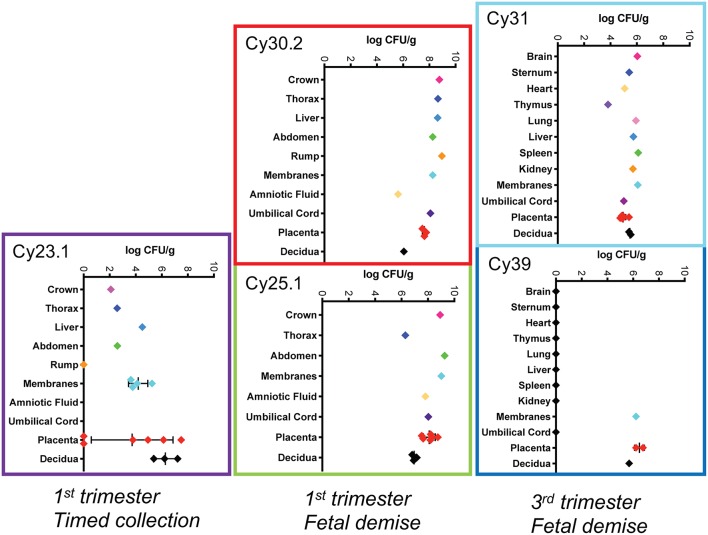
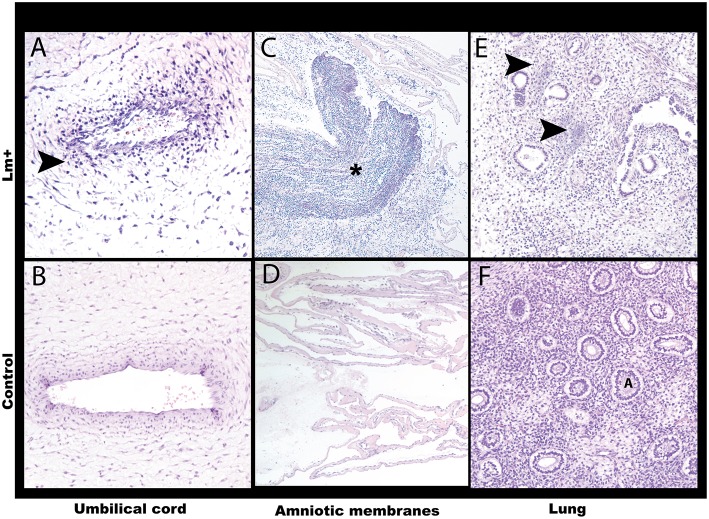
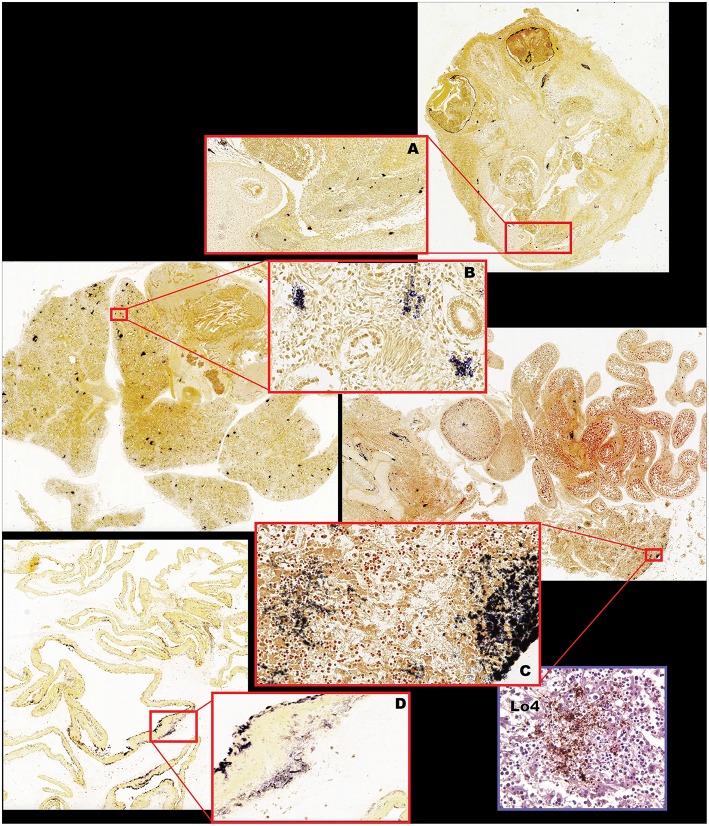
Listeria monocytogenes (Lm) is a common environmental bacterium that thrives on vegetation and soil matter, but can infect humans if contaminated food products are ingested, resulting in severe disease in immunosuppressed populations, including pregnant women and newborns. To better understand how the unique immunological milieu of pregnancy increases susceptibility to infection, we study listeriosis in cynomolgus macaques, a non-human primate that closely resembles humans in placentation and in the physiology, and immunology of pregnancy. Non-human primates are naturally susceptible to Lm infection, and spontaneous abortions due to listeriosis are known to occur in outdoor macaque colonies, making them ideal models to understand the disease pathogenesis and host-pathogen relationship of listeriosis. We have previously shown that Lm infection in the first trimester has a high rate of miscarriage. This study expands on our previous findings by assessing how the quantity of Lm as well as stage of pregnancy at the time of exposure may influence disease susceptibility. In the current study we inoculated a cohort of macaques with a lower dose of Lm than our previous study and although this did not result in fetal demise, there was evidence of in utero inflammation and fetal distress. Animals that were reinfected with an equivalent or higher dose of the same strain of Lm resulted in approximately half of cases continuing to term and half ending in fetal demise. These cases had inconsistent bacterial colonization of the fetal compartment, suggesting that Lm does not need to directly infect the placenta to cause adverse pregnancy outcomes. Timed surgical collection of tissues following inoculation demonstrated that transmission from mother to fetus can occur as soon as 5 days post-inoculation. Lastly, third trimester inoculation resulted in pregnancy loss in 3 out of 4 macaques, accompanied by characteristic pathology and Lm colonization. Collectively, our studies demonstrate that common laboratory culture tests may not always recover Lm despite known maternal ingestion. Notably, we also find it is possible for maternal infection to resolve in some cases with no discernible adverse outcome; however, such cases had evidence of a sterile intrauterine inflammatory response, with unknown consequences for fetal development.
Keywords: cytokines; fetal infection; histopathology; listeriosis; non-human primate; pregnancy.
Copyright © 2019 Wolfe, Kerr, Mejia, Simmons, Czuprynski and Golos.
Figures
Similar articles
-
Acute Fetal Demise with First Trimester Maternal Infection Resulting from Listeria monocytogenes in a Nonhuman Primate Model.mBio. 2017 Feb 21;8(1):e01938-16. doi: 10.1128/mBio.01938-16. mBio. 2017. PMID: 28223455 Free PMC article.
-
Listeria monocytogenes infection in pregnant macaques alters the maternal gut microbiome†.Biol Reprod. 2023 Nov 15;109(5):618-634. doi: 10.1093/biolre/ioad104. Biol Reprod. 2023. PMID: 37665249 Free PMC article.
-
[Placenta-specific virulence factors involved in Listeria monocytogenes infection].Sheng Wu Gong Cheng Xue Bao. 2022 Jun 25;38(6):2139-2152. doi: 10.13345/j.cjb.210860. Sheng Wu Gong Cheng Xue Bao. 2022. PMID: 35786468 Review. Chinese.
-
Perinatal Listeria monocytogenes susceptibility despite preconceptual priming and maintenance of pathogen-specific CD8(+) T cells during pregnancy.Cell Mol Immunol. 2014 Nov;11(6):595-605. doi: 10.1038/cmi.2014.84. Epub 2014 Sep 22. Cell Mol Immunol. 2014. PMID: 25242275 Free PMC article.
-
Pregnancy-related listeriosis.Birth Defects Res. 2017 Mar 15;109(5):324-335. doi: 10.1002/bdr2.1012. Birth Defects Res. 2017. PMID: 28398675 Review.
Cited by
-
The promise of placental extracellular vesicles: models and challenges for diagnosing placental dysfunction in utero†.Biol Reprod. 2021 Jan 4;104(1):27-57. doi: 10.1093/biolre/ioaa152. Biol Reprod. 2021. PMID: 32856695 Free PMC article. Review.
-
Infections at the maternal-fetal interface: an overview of pathogenesis and defence.Nat Rev Microbiol. 2022 Feb;20(2):67-82. doi: 10.1038/s41579-021-00610-y. Epub 2021 Aug 25. Nat Rev Microbiol. 2022. PMID: 34433930 Free PMC article. Review.
-
The Viable But Non-Culturable State of Listeria monocytogenes in the One-Health Continuum.Front Cell Infect Microbiol. 2022 Mar 18;12:849915. doi: 10.3389/fcimb.2022.849915. eCollection 2022. Front Cell Infect Microbiol. 2022. PMID: 35372114 Free PMC article. Review.
-
Acute Exposure to the Food-Borne Pathogen Listeria monocytogenes Does Not Induce α-Synuclein Pathology in the Colonic ENS of Nonhuman Primates.J Inflamm Res. 2021 Dec 22;14:7265-7279. doi: 10.2147/JIR.S337549. eCollection 2021. J Inflamm Res. 2021. PMID: 34992416 Free PMC article.
-
Profiling of rhizosphere-associated microbial communities in North Alabama soils infested with varied levels of reniform nematodes.Front Plant Sci. 2025 Mar 7;16:1521579. doi: 10.3389/fpls.2025.1521579. eCollection 2025. Front Plant Sci. 2025. PMID: 40123958 Free PMC article.
References
-
- Bortolussi R., Mailman T. L. (2011). Infectious Diseases of the Fetus and Newborn. 7th ed Philadelphia, PA: Elsevier Saunders.
-
- Centers for Disease Control Prevention (2016). Listeriosis Information for Health Professionals and Laboratories. Available online at: https://www.cdc.gov/listeria/technical.html (accessed December 12, 2016).
-
- Centers for Disease Control Prevention (2019). Prevent Infections During Pregnancy. Available online at: https://www.cdc.gov/features/prenatalinfections/index.html (accessed June 19. 2019).
Grants and funding
LinkOut - more resources
Full Text Sources