

Host Components Contributing to Respiratory Syncytial Virus Pathogenesis
- PMID: 31572372
- PMCID: PMC6753334
- DOI: 10.3389/fimmu.2019.02152
Host Components Contributing to Respiratory Syncytial Virus Pathogenesis
Abstract
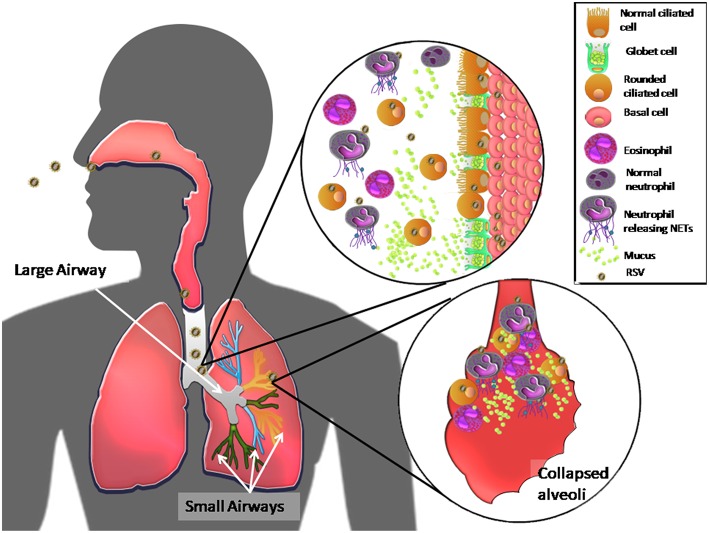
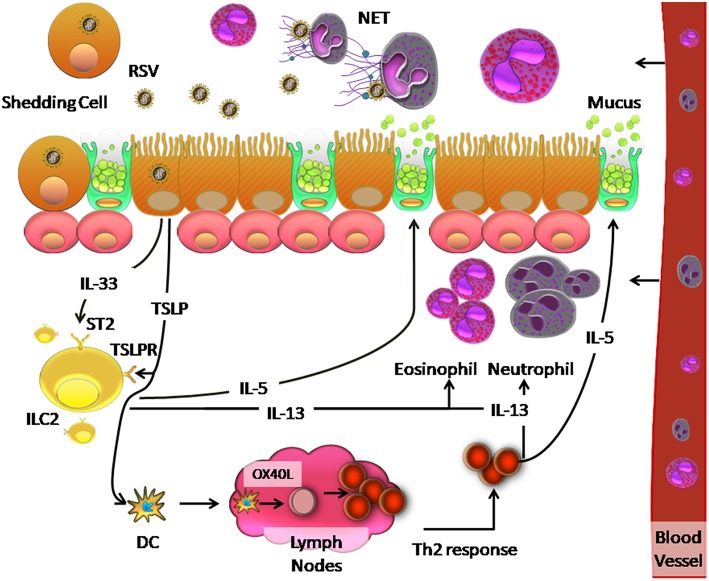
Respiratory syncytial virus (RSV) is the most prevalent viral etiological agent of acute respiratory tract infection. Although RSV affects people of all ages, the disease is more severe in infants and causes significant morbidity and hospitalization in young children and in the elderly. Host factors, including an immature immune system in infants, low lymphocyte levels in patients under 5 years old, and low levels of RSV-specific neutralizing antibodies in the blood of adults over 65 years of age, can explain the high susceptibility to RSV infection in these populations. Other host factors that correlate with severe RSV disease include high concentrations of proinflammatory cytokines such as interleukins (IL)-6, IL-8, tumor necrosis factor (TNF)-α, and thymic stromal lymphopoitein (TSLP), which are produced in the respiratory tract of RSV-infected individuals, accompanied by a strong neutrophil response. In addition, data from studies of RSV infections in humans and in animal models revealed that this virus suppresses adaptive immune responses that could eliminate it from the respiratory tract. Here, we examine host factors that contribute to RSV pathogenesis based on an exhaustive review of in vitro infection in humans and in animal models to provide insights into the design of vaccines and therapeutic tools that could prevent diseases caused by RSV.
Keywords: RSV; disease; host factors; innate and adaptive immune response; pathogenesis.
Copyright © 2019 Carvajal, Avellaneda, Salazar-Ardiles, Maya, Kalergis and Lay.
Figures
Similar articles
-
Respiratory Syncytial Virus (RSV) Pulmonary Infection in Humanized Mice Induces Human Anti-RSV Immune Responses and Pathology.J Virol. 2016 Apr 29;90(10):5068-5074. doi: 10.1128/JVI.00259-16. Print 2016 May 15. J Virol. 2016. PMID: 26962219 Free PMC article.
-
Antibody and Local Cytokine Response to Respiratory Syncytial Virus Infection in Community-Dwelling Older Adults.mSphere. 2020 Sep 2;5(5):e00577-20. doi: 10.1128/mSphere.00577-20. mSphere. 2020. PMID: 32878928 Free PMC article.
-
Impaired immune response in severe human lower tract respiratory infection by respiratory syncytial virus.Pediatr Infect Dis J. 2009 Oct;28(10):867-73. doi: 10.1097/INF.0b013e3181a3ea71. Pediatr Infect Dis J. 2009. PMID: 19738511
-
New insights on the viral and host factors contributing to the airway pathogenesis caused by the respiratory syncytial virus.Crit Rev Microbiol. 2016 Sep;42(5):800-12. doi: 10.3109/1040841X.2015.1055711. Epub 2015 Jun 29. Crit Rev Microbiol. 2016. PMID: 26119025 Review.
-
The adaptive immune response to respiratory syncytial virus.Curr Top Microbiol Immunol. 2013;372:155-71. doi: 10.1007/978-3-642-38919-1_8. Curr Top Microbiol Immunol. 2013. PMID: 24362689 Review.
Cited by
-
The Role of Dendritic Cells During Infections Caused by Highly Prevalent Viruses.Front Immunol. 2020 Jul 16;11:1513. doi: 10.3389/fimmu.2020.01513. eCollection 2020. Front Immunol. 2020. PMID: 32765522 Free PMC article. Review.
-
Respiratory Syncytial Virus: A Comprehensive Review of Transmission, Pathophysiology, and Manifestation.Cureus. 2023 Mar 18;15(3):e36342. doi: 10.7759/cureus.36342. eCollection 2023 Mar. Cureus. 2023. PMID: 37082497 Free PMC article. Review.
-
The role of goblet cells in viral pathogenesis.FEBS J. 2021 Dec;288(24):7060-7072. doi: 10.1111/febs.15731. Epub 2021 Feb 9. FEBS J. 2021. PMID: 33507606 Free PMC article. Review.
-
Role of Extracellular Trap Release During Bacterial and Viral Infection.Front Microbiol. 2022 Jan 26;13:798853. doi: 10.3389/fmicb.2022.798853. eCollection 2022. Front Microbiol. 2022. PMID: 35154050 Free PMC article. Review.
-
Beyond the first breath: comprehensive respiratory syncytial virus prevention through maternal immunization and infant immunoprophylaxis.Asian Biomed (Res Rev News). 2025 Jul 28;19(3):116-130. doi: 10.2478/abm-2025-0015. eCollection 2025 Jun. Asian Biomed (Res Rev News). 2025. PMID: 40735667 Free PMC article. Review.
References
-
- Iwane MK, Edwards KM, Szilagyi PG, Walker FJ, Griffin MR, Weinberg GA, et al. Population-based surveillance for hospitalizations associated with respiratory syncytial virus, influenza virus, and parainfluenza viruses among young children. Pediatrics. (2004) 113:1758–64. 10.1542/peds.113.6.1758 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical