

Microbial Translocation Is Linked to a Specific Immune Activation Profile in HIV-1-Infected Adults With Suppressed Viremia
- PMID: 31572392
- PMCID: PMC6753629
- DOI: 10.3389/fimmu.2019.02185
Microbial Translocation Is Linked to a Specific Immune Activation Profile in HIV-1-Infected Adults With Suppressed Viremia
Abstract
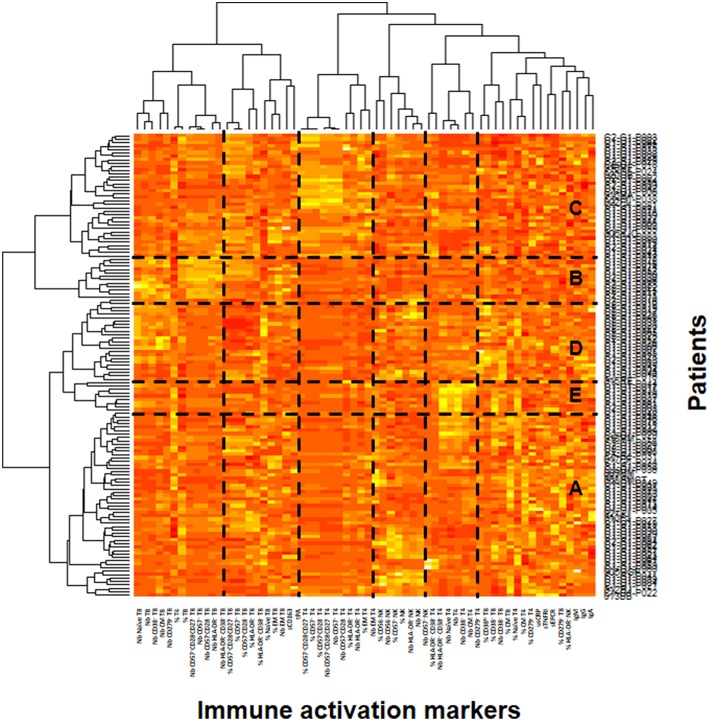
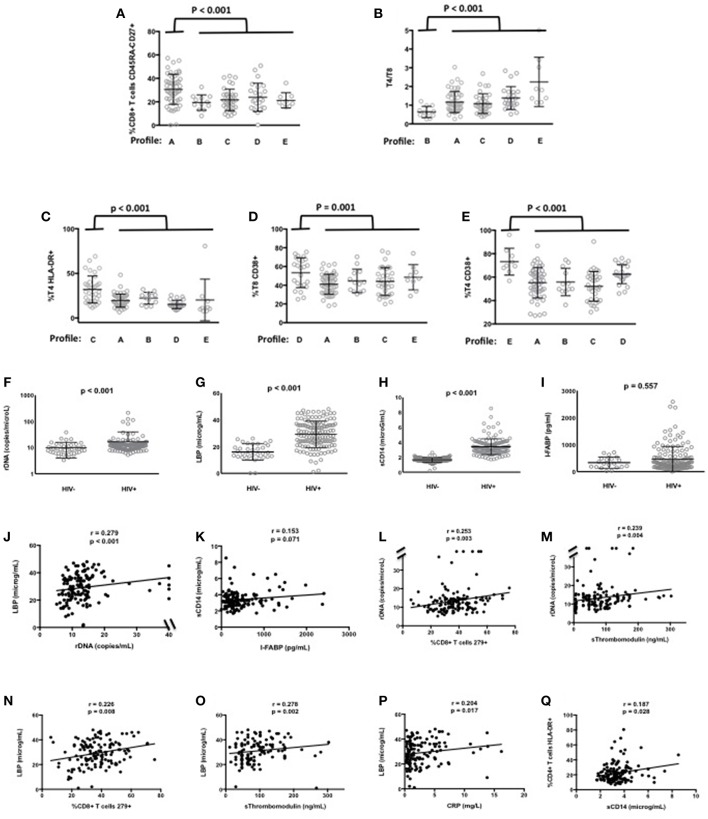
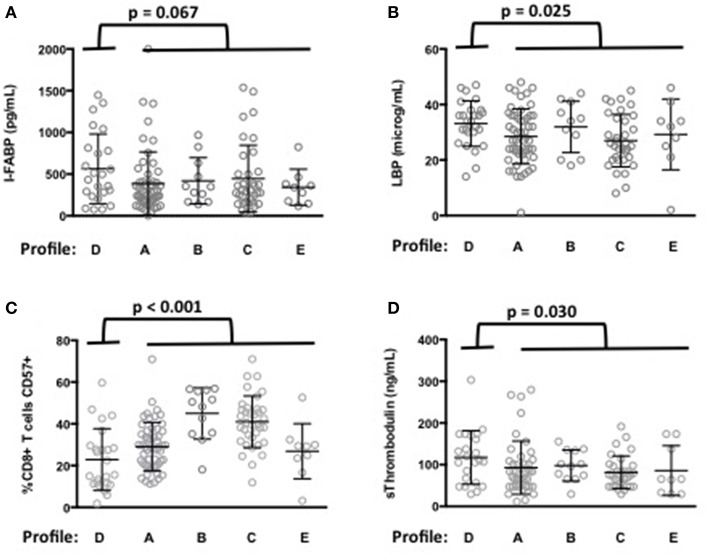
Persistent immune activation in virologically suppressed HIV-1 patients, which may be the consequence of various factors including microbial translocation, is a major cause of comorbidities. We have previously shown that different profiles of immune activation may be distinguished in virological responders. Here, we tested the hypothesis that a particular profile might be the consequence of microbial translocation. To this aim, we measured 64 soluble and cell surface markers of inflammation and CD4+ and CD8+ T-cell, B cell, monocyte, NK cell, and endothelial activation in 140 adults under efficient antiretroviral therapy, and classified patients and markers using a double hierarchical clustering analysis. We also measured the plasma levels of the microbial translocation markers bacterial DNA, lipopolysaccharide binding protein (LBP), intestinal-fatty acid binding protein, and soluble CD14. We identified five different immune activation profiles. Patients with an immune activation profile characterized by a high percentage of CD38+CD8+ T-cells and a high level of the endothelial activation marker soluble Thrombomodulin, presented with higher LBP mean (± SEM) concentrations (33.3 ± 1.7 vs. 28.7 ± 0.9 μg/mL, p = 0.025) than patients with other profiles. Our data are consistent with the hypothesis that the immune activation profiles we described are the result of different etiological factors. We propose a model, where particular causes of immune activation, as microbial translocation, drive particular immune activation profiles responsible for particular comorbidities.
Keywords: bacterial translocation; cell activation; coagulation; endothelium; inflammation.
Copyright © 2019 Younas, Psomas, Reynes, Cezar, Kundura, Portales, Merle, Atoui, Fernandez, Le Moing, Barbuat, Moranne, Sotto, Sabatier, Fabbro, Vincent, Dunyach-Remy, Winter, Reynes, Lavigne and Corbeau.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous