

Consensus recommendations for management of patients with type 2 diabetes mellitus and cardiovascular diseases
- PMID: 31572499
- PMCID: PMC6761728
- DOI: 10.1186/s13098-019-0476-0
Consensus recommendations for management of patients with type 2 diabetes mellitus and cardiovascular diseases
Abstract
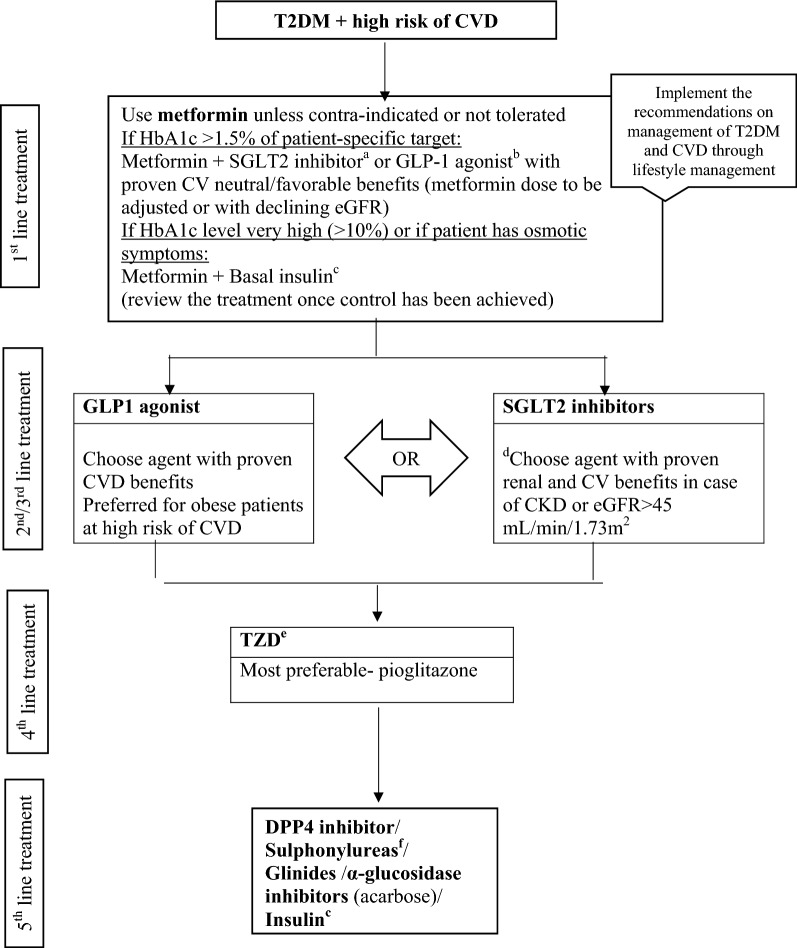
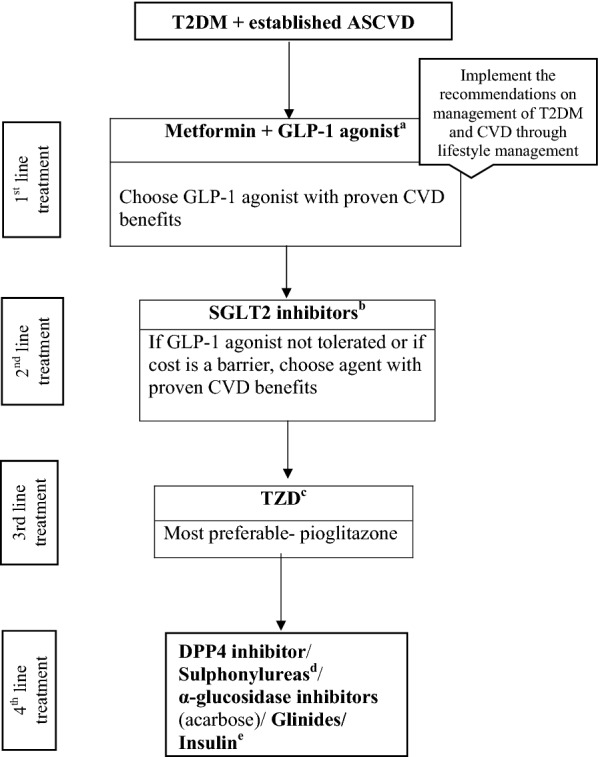
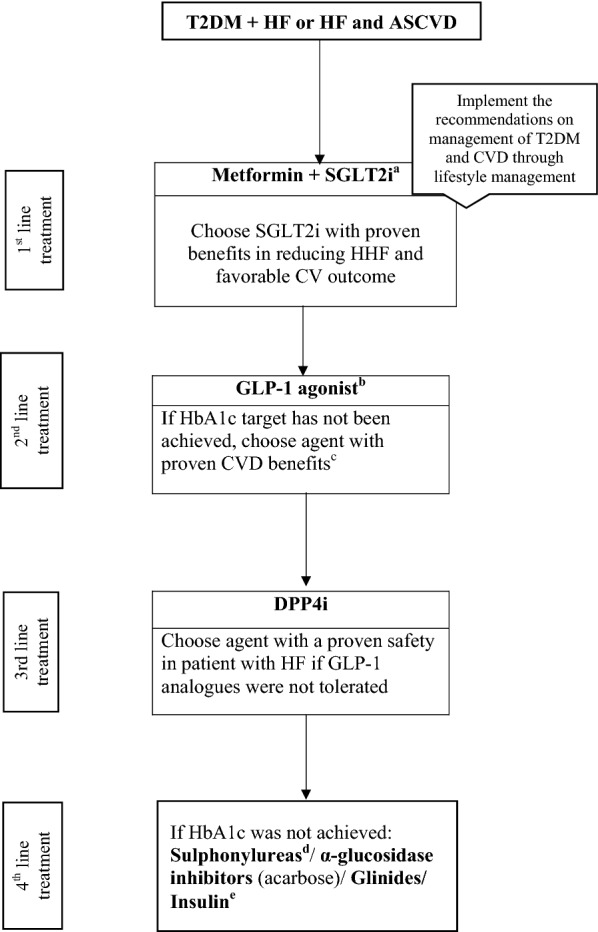
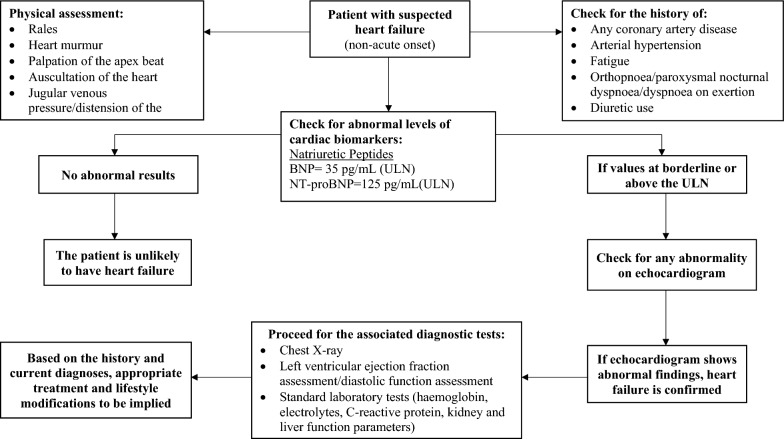
The recent American Diabetes Association and the European Association for the Study of Diabetes guideline mentioned glycaemia management in type 2 diabetes mellitus (T2DM) patients with cardiovascular diseases (CVDs); however, it did not cover the treatment approaches for patients with T2DM having a high risk of CVD, and treatment and screening approaches for CVDs in patients with concomitant T2DM. This consensus guideline undertakes the data obtained from all the cardiovascular outcome trials (CVOTs) to propose approaches for the T2DM management in presence of CV comorbidities. For patients at high risk of CVD, metformin is the drug of choice to manage the T2DM to achieve a patient specific HbA1c target. In case of established CVD, a combination of glucagon-like peptide-1 receptor agonist with proven CV benefits is recommended along with metformin, while for chronic kidney disease or heart failure, a sodium-glucose transporter proteins-2 inhibitor with proven benefit is advised. This document also summarises various screening and investigational approaches for the major CV events with their accuracy and specificity along with the treatment guidance to assist the healthcare professionals in selecting the best management strategies for every individual. Since lifestyle modification and management plays an important role in maintaining the effectiveness of the pharmacological therapies, authors of this consensus recommendation have also briefed on the patient-centric non-pharmacological management of T2DM and CVD.
Keywords: CVDs; CVOTs; Consensus; HF; T2DM.
© The Author(s) 2019.
Conflict of interest statement
Competing interestsThe authors declare that they have no competing interests.
Figures
References
-
- International Diabetes Federation: IDF diabetes atlas seventh edition. 2015.
-
- International Diabetes Federation: Diabetes and cardiovascular disease. 2016.
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
