

Characterizing the Human Immunodeficiency Virus Care Continuum Among Transgender Women and Cisgender Women and Men in Clinical Care: A Retrospective Time-series Analysis
- PMID: 31573601
- PMCID: PMC7319059
- DOI: 10.1093/cid/ciz322
Characterizing the Human Immunodeficiency Virus Care Continuum Among Transgender Women and Cisgender Women and Men in Clinical Care: A Retrospective Time-series Analysis
Abstract
Background: Prior studies suggest that transgender women (TW) with human immunodeficiency virus (HIV) are less likely to be virally suppressed than cisgender women (CW) and cisgender men (CM). However, prior data are limited by small sample sizes and cross-sectional designs. We sought to characterize the HIV care continuum comparing TW to CW and CM in the United States and Canada.
Methods: We analyzed annual HIV care continuum outcomes by gender status from January 2001 through December 2015 among adults (aged ≥18 years) in 15 clinical cohorts. Outcomes were retention in care and viral suppression.
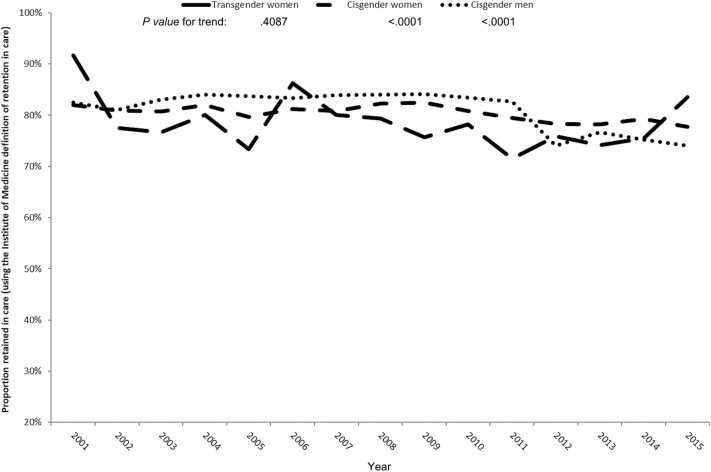
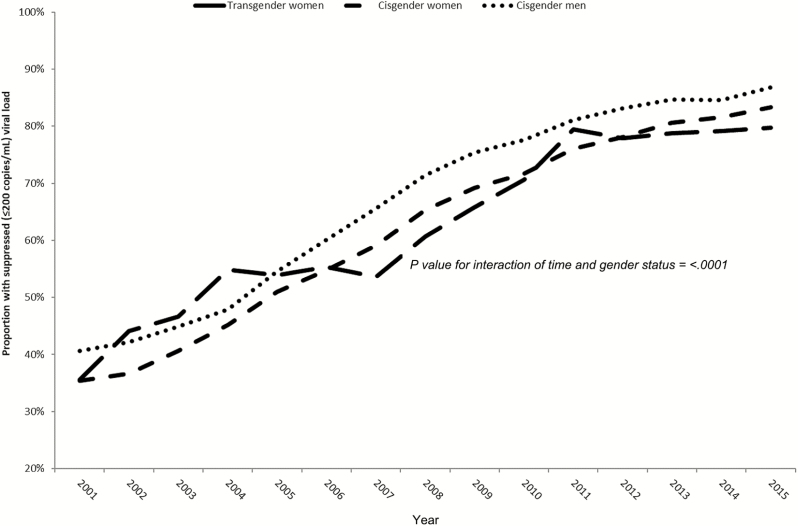
Results: The study population included TW (n = 396), CW (n = 14 094), and CM (n = 101 667). TW had lower proportions retained in care than CW and CM (P < .01). Estimates of retention in care were consistently lower in TW, with little change over time within each group. TW and CW had similar proportions virally suppressed over time (TW, 36% in 2001 and 80% in 2015; CW, 35% in 2001 and 83% in 2015) and were lower than CM (41% in 2001 and 87% in 2015). These differences did not reach statistical significance after adjusting for age, race, HIV risk group, and cohort.
Conclusions: TW experience challenges with retention in HIV care. However, TW who are engaged in care achieve viral suppression that is comparable to that of CW and CM of similar age, race, and HIV risk group. Further research is needed to understand care engagement disparities.
Keywords: HIV continuum of care; HIV viral suppression; retention in care; transgender women.
© The Author(s) 2019. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Figures
References
-
- Baral SD, Poteat T, Strömdahl S, Wirtz AL, Guadamuz TE, Beyrer C. Worldwide burden of HIV in transgender women: a systematic review and meta-analysis. Lancet Infect Dis 2013; 13:214–22. - PubMed
Publication types
MeSH terms
Grants and funding
- U01 AI035039/AI/NIAID NIH HHS/United States
- K24 DA000432/DA/NIDA NIH HHS/United States
- P30 AI110527/AI/NIAID NIH HHS/United States
- HCP-97105/CIHR/Canada
- U01 AI031834/AI/NIAID NIH HHS/United States
- U01 AI103397/AI/NIAID NIH HHS/United States
- P30 AI027757/AI/NIAID NIH HHS/United States
- Z01 CP010176/ImNIH/Intramural NIH HHS/United States
- KL2 TR000421/TR/NCATS NIH HHS/United States
- U01 AI037984/AI/NIAID NIH HHS/United States
- K23 EY013707/EY/NEI NIH HHS/United States
- U01 AI035004/AI/NIAID NIH HHS/United States
- R01 DA012568/DA/NIDA NIH HHS/United States
- U01 AA020790/AA/NIAAA NIH HHS/United States
- R01 CA165937/CA/NCI NIH HHS/United States
- U01 AI037613/AI/NIAID NIH HHS/United States
- P30 MH062246/MH/NIMH NIH HHS/United States
- Z01 CP010121/ImNIH/Intramural NIH HHS/United States
- U01 AI035040/AI/NIAID NIH HHS/United States
- F31 DA037788/DA/NIDA NIH HHS/United States
- U10 EY008057/EY/NEI NIH HHS/United States
- TGF-96118/CIHR/Canada
- U01 DA036935/DA/NIDA NIH HHS/United States
- U01 AI035041/AI/NIAID NIH HHS/United States
- U01 AI038855/AI/NIAID NIH HHS/United States
- F31 AI124794/AI/NIAID NIH HHS/United States
- N02CP55504/CP/NCI NIH HHS/United States
- R01 AG053100/AG/NIA NIH HHS/United States
- U24 AA020794/AA/NIAAA NIH HHS/United States
- P30 AI094189/AI/NIAID NIH HHS/United States
- G12 MD007583/MD/NIMHD NIH HHS/United States
- U10 EY008052/EY/NEI NIH HHS/United States
- KL2 TR001077/TR/NCATS NIH HHS/United States
- U01 HD032632/HD/NICHD NIH HHS/United States
- CBR-94036/CIHR/Canada
- U01 AA013566/AA/NIAAA NIH HHS/United States
- U10 EY008067/EY/NEI NIH HHS/United States
- K01 AI093197/AI/NIAID NIH HHS/United States
- U54 MD007587/MD/NIMHD NIH HHS/United States
- P30 AI027767/AI/NIAID NIH HHS/United States
- U01 AI103401/AI/NIAID NIH HHS/United States
- U01 AI038858/AI/NIAID NIH HHS/United States
- R01 DA011602/DA/NIDA NIH HHS/United States
- U01 AI035042/AI/NIAID NIH HHS/United States
- K24 AI065298/AI/NIAID NIH HHS/United States
- U01 AI103408/AI/NIAID NIH HHS/United States
- K24 AI118591/AI/NIAID NIH HHS/United States
- U01 AI034989/AI/NIAID NIH HHS/United States
- U01 AI034993/AI/NIAID NIH HHS/United States
- P30 AI027763/AI/NIAID NIH HHS/United States
- R01 AA016893/AA/NIAAA NIH HHS/United States
- M01 RR000052/RR/NCRR NIH HHS/United States
- CBR-86906/CIHR/Canada
- U01 AI042590/AI/NIAID NIH HHS/United States
- U01 AI034994/AI/NIAID NIH HHS/United States
- K01 AI131895/AI/NIAID NIH HHS/United States
- UM1 AI035043/AI/NIAID NIH HHS/United States
- U01 AI069918/AI/NIAID NIH HHS/United States
- P30 AI036219/AI/NIAID NIH HHS/United States
- R24 AI067039/AI/NIAID NIH HHS/United States
- P30 AI050410/AI/NIAID NIH HHS/United States
- K01 HL137557/HL/NHLBI NIH HHS/United States
