

Effects of rosuvastatin on the immune system in healthy volunteers with normal serum cholesterol
- PMID: 31573980
- PMCID: PMC6948773
- DOI: 10.1172/jci.insight.131530
Effects of rosuvastatin on the immune system in healthy volunteers with normal serum cholesterol
Abstract
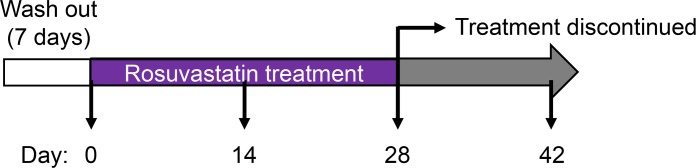
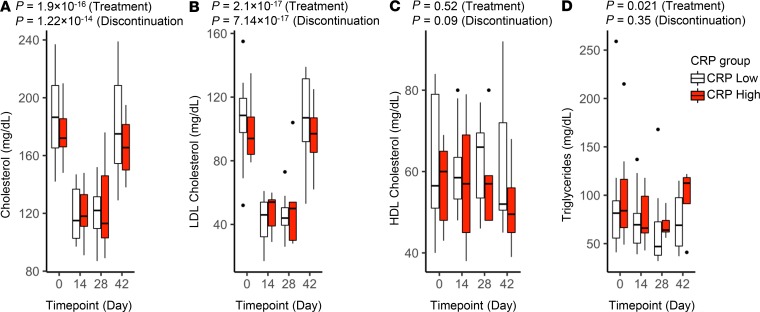
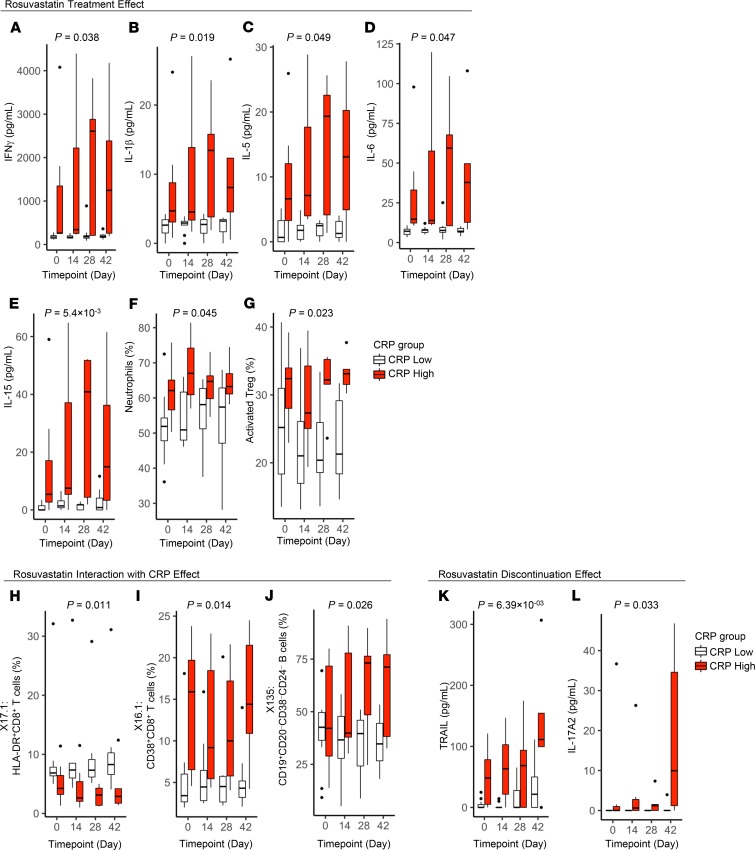
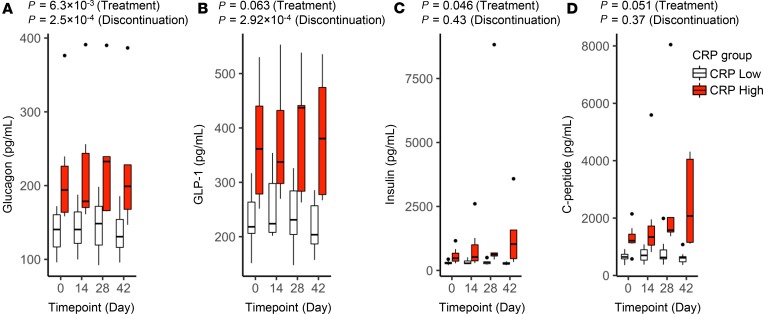
BACKGROUNDHMG-CoA reductase inhibitors (statins) are prescribed to millions of people. Statins are antiinflammatory independent of their cholesterol-reducing effects. To date, most reports on the immune effects of statins have assayed a narrow array of variables and have focused on cell lines, rodent models, or patient cohorts. We sought to define the effect of rosuvastatin on the "immunome" of healthy, normocholesterolemic subjects.METHODSWe conducted a prospective study of rosuvastatin (20 mg/d × 28 days) in 18 statin-naive adults with LDL cholesterol <130 mg/dL. A panel of >180 immune/biochemical/endocrinologic variables was measured at baseline and on days 14, 28, and 42 (14 days after drug withdrawal). Drug effect was evaluated using linear mixed-effects models. Potential interactions between drug and baseline high-sensitivity C-reactive protein (hsCRP) were evaluated.RESULTSA wide array of immune measures changed (nominal P < 0.05) during rosuvastatin treatment, although the changes were modest in magnitude, and few met an FDR of 0.05. Among changes noted were a concordant increase in proinflammatory cytokines (IFN-γ, IL-1β, IL-5, IL-6, and TNF-α) and peripheral blood neutrophil frequency, and a decline in activated Treg frequency. Several drug effects were significantly modified by baseline hsCRP, and some did not resolve after drug withdrawal. Among other unexpected rosuvastatin effects were changes in erythrocyte indices, glucose-regulatory hormones, CD8+ T cells, and haptoglobin.CONCLUSIONRosuvastatin induces modest changes in immunologic and metabolic measures in normocholesterolemic subjects, with several effects dependent on baseline CRP. Future, larger studies are warranted to validate these changes and their physiological significance.TRIAL REGISTRATIONClinicalTrials.gov NCT01200836.FUNDINGThis research was supported by the Intramural Research Program of the NIH, National Institute of Environmental Health Sciences (Z01 ES102005), and the trans-NIH Center for Human Immunology.
Keywords: Cellular immune response; Cholesterol; Clinical Trials; Cytokines; Immunology.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
