

Preconception diabetes mellitus and adverse pregnancy outcomes in over 6.4 million women: A population-based cohort study in China
- PMID: 31574092
- PMCID: PMC6771981
- DOI: 10.1371/journal.pmed.1002926
Preconception diabetes mellitus and adverse pregnancy outcomes in over 6.4 million women: A population-based cohort study in China
Abstract
Background: Diabetes mellitus (DM) increases the risk of adverse maternal and neonatal outcomes, and optimization of glycemic control during pregnancy can help mitigate risks associated with diabetes. However, studies seldom focus precisely on maternal blood glucose level prior to pregnancy. We aimed to evaluate the associations between preconception blood fasting plasma glucose (FPG) level and subsequent pregnancy outcomes.
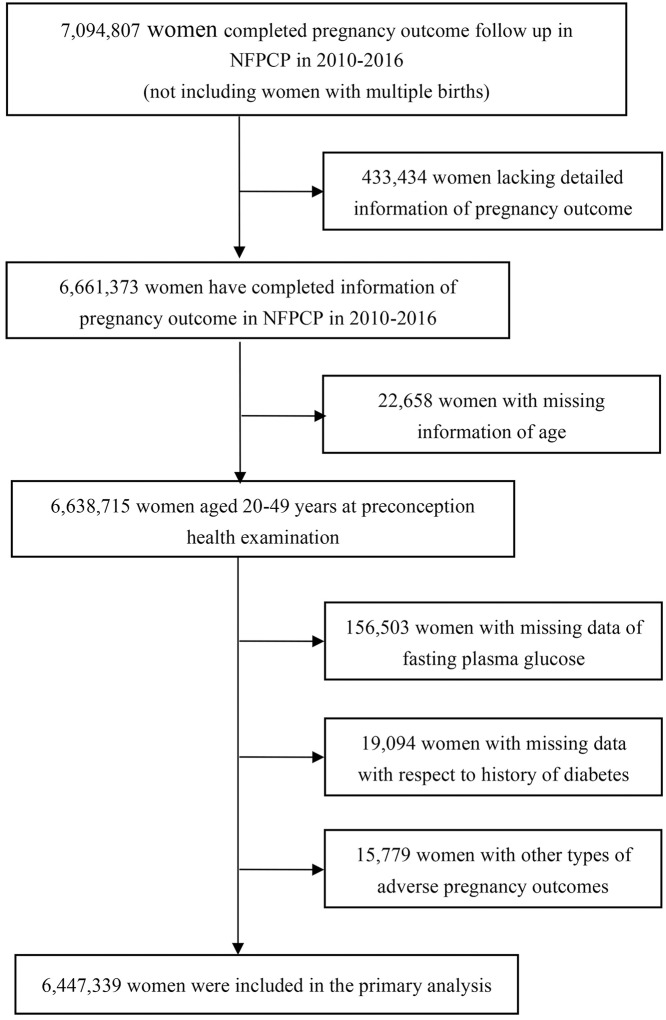
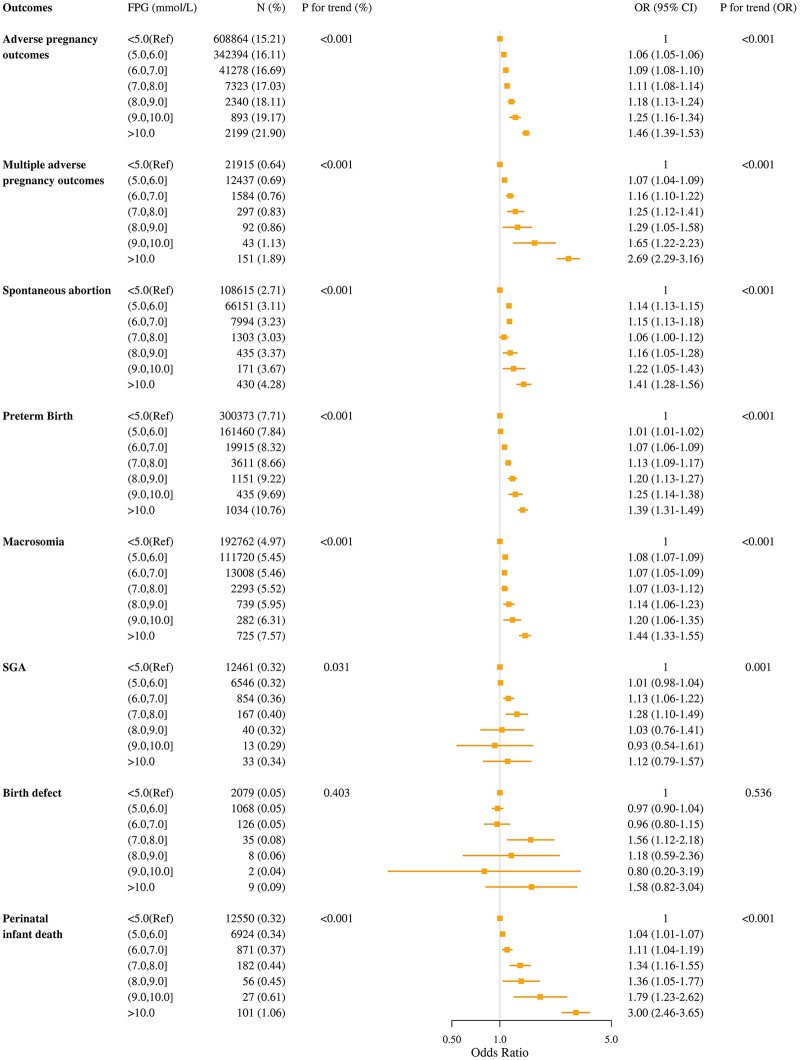
Methods and findings: We conducted a population-based retrospective cohort study among 6,447,339 women aged 20-49 years old who participated in National Free Pre-Pregnancy Checkups Project and completed pregnancy outcomes follow-up between 2010 and 2016 in China. During the preconception health examination, serum FPG concentration was measured, and self-reported history of DM was collected. Women were classified into three groups (normal FPG group: FPG < 5.6 mmol/L and no self-reported history of DM; impaired fasting glucose [IFG]: FPG 5.6-6.9 mmol/L and no self-reported history of DM; and DM: FPG ≥ 7.0 mmol/L or self-reported history of DM). The primary outcomes were adverse pregnancy outcomes, including spontaneous abortion, preterm birth (PTB), macrosomia, small for gestational age infant (SGA), birth defect, and perinatal infant death. Logistic regression model was used to calculate odds ratio (OR) and 95% confidence interval (CI) after adjusting for confounding variables. The mean age of women was 25.24 years, 91.47% were of Han nationality, and 92.85% were from rural areas. The incidence of DM and IFG was 1.18% (76,297) and 13.15% (847,737), respectively. Only 917 (1.20%) women reported a history of DM (awareness of their DM status), of whom 37.28% (337) had an elevated preconception FPG level (≥ 5.6 mmol/L), regarded as noncontrolled DM. A total of 1,005,568 (15.60%) women had adverse pregnancy outcomes. Compared with women with normal FPG, women with IFG had higher risks of spontaneous abortion (OR 1.08; 95% CI 1.06-1.09; P < 0.001), PTB (1.02; 1.01-1.03; P < 0.001), macrosomia (1.07; 1.06-1.08; P < 0.001), SGA (1.06; 1.02-1.10; P = 0.007), and perinatal infant death (1.08; 1.03-1.12; P < 0.001); the corresponding ORs for women with DM were 1.11 (95% CI 1.07-1.15; P < 0.001), 1.17 (1.14-1.20; P < 0.001), 1.13 (1.09-1.16; P < 0.001), 1.17 (1.04-1.32; P = 0.008), and 1.59 (1.44-1.76; P < 0.001). Women with DM also had a higher risk of birth defect (OR 1.42; 95% CI 1.15-1.91; P = 0.002). Among women without self-reported history of DM, there was a positive linear association between FPG levels and spontaneous abortion, PTB, macrosomia, SGA, and perinatal infant death (P for trend <0.001, <0.001, <0.001, 0.001, <0.001). Information about hypoglycemic medication before or during pregnancy was not collected, and we cannot adjust it in the analysis, which could result in underestimation of risks. Data on 2-hour plasma glucose level and HbA1c concentration were not available, and the glycemic control status was evaluated according to FPG value in women with DM.
Conclusions: Women with preconception IFG or DM had higher risk of adverse pregnancy outcomes, including spontaneous abortion, PTB, macrosomia, SGA, and perinatal infant death. Preconception glycemic control through appropriate methods is one of the most important aspects of preconception care and should not be ignored by policy makers.
Conflict of interest statement
I have read the journal’s policy and the authors of this manuscript have the following competing interests: Professor Huixia Yang is a guest editor for the Maternal and Child Health & Nutrition Special Issue.
Figures
Similar articles
-
Preconception hypoglycemia and adverse pregnancy outcomes in Chinese women aged 20-49 years: A retrospective cohort study in China.PLoS Med. 2025 Jul 29;22(7):e1004667. doi: 10.1371/journal.pmed.1004667. eCollection 2025 Jul. PLoS Med. 2025. PMID: 40729125 Free PMC article.
-
Preconception Thyrotropin Levels and Risk of Adverse Pregnancy Outcomes in Chinese Women Aged 20 to 49 Years.JAMA Netw Open. 2021 Apr 1;4(4):e215723. doi: 10.1001/jamanetworkopen.2021.5723. JAMA Netw Open. 2021. PMID: 33847747 Free PMC article.
-
Maternal fasting glucose levels throughout the pregnancy and risk of adverse birth outcomes in newborns: a birth cohort study in Foshan city, Southern China.Eur J Endocrinol. 2023 Jan 10;188(1):lvac019. doi: 10.1093/ejendo/lvac019. Eur J Endocrinol. 2023. PMID: 36680781
-
Systematic review and meta-analysis of the effectiveness of pre-pregnancy care for women with diabetes for improving maternal and perinatal outcomes.PLoS One. 2020 Aug 18;15(8):e0237571. doi: 10.1371/journal.pone.0237571. eCollection 2020. PLoS One. 2020. PMID: 32810195 Free PMC article.
-
First-trimester fasting plasma glucose as a predictor of subsequent gestational diabetes mellitus and adverse fetomaternal outcomes: A systematic review and meta-analysis.Diabetes Metab Syndr. 2024 Jun;18(6):103051. doi: 10.1016/j.dsx.2024.103051. Epub 2024 Jun 1. Diabetes Metab Syndr. 2024. PMID: 38843646
Cited by
-
Pregnancy in Patients with Type One Diabetes Mellitus Treated with Continuous Subcutaneous Insulin Infusion-Preconception Basal Insulin Dose as a Potential Risk Factor for Fetal Overgrowth?Int J Environ Res Public Health. 2020 Sep 9;17(18):6566. doi: 10.3390/ijerph17186566. Int J Environ Res Public Health. 2020. PMID: 32916984 Free PMC article.
-
A retrospective study on the impact of the timing of diabetes diagnosis on maternal and fetal outcomes.Arch Gynecol Obstet. 2025 May 30. doi: 10.1007/s00404-025-08047-x. Online ahead of print. Arch Gynecol Obstet. 2025. PMID: 40445207
-
Non-Pharmacological Management of Gestational Diabetes Mellitus with a High Fasting Glycemic Parameter: A Hospital-Based Study in Vietnam.J Clin Med. 2024 Oct 2;13(19):5895. doi: 10.3390/jcm13195895. J Clin Med. 2024. PMID: 39407955 Free PMC article.
-
2. Classification and Diagnosis of Diabetes: Standards of Care in Diabetes-2023.Diabetes Care. 2023 Jan 1;46(Suppl 1):S19-S40. doi: 10.2337/dc23-S002. Diabetes Care. 2023. PMID: 36507649 Free PMC article. Review.
-
Dose-response association between maternal smoking during pregnancy and the risk of infant death: a nationwide, population-based, retrospective cohort study.EClinicalMedicine. 2023 Feb 26;57:101858. doi: 10.1016/j.eclinm.2023.101858. eCollection 2023 Mar. EClinicalMedicine. 2023. PMID: 36879656 Free PMC article.
References
-
- Danaei G, Finucane MM, Lu Y, Singh GM, Cowan MJ, Paciorek CJ, et al. National, regional, and global trends in fasting plasma glucose and diabetes prevalence since 1980: systematic analysis of health examination surveys and epidemiological studies with 370 country-years and 2.7 million participants. Lancet. 2011;378(9785):31–40. 10.1016/S0140-6736(11)60679-X - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
