

Surgical treatment of malignant paraganglioma with spinal invasion in a juvenile patient: A case report
- PMID: 31574816
- PMCID: PMC6775344
- DOI: 10.1097/MD.0000000000017145
Surgical treatment of malignant paraganglioma with spinal invasion in a juvenile patient: A case report
Abstract
Rationale: Paragangliomas are rare neuroendocrine tumors that originate in specialized cells derived from the neural crest with metastasis to the thoracic spine being among the rarest forms. Here, we are presenting a detailed analysis of a case of malignant paraganglioma in the thoracic spinal region in a 14-year-old boy. Our focus is to emphasize the importance of considering malignant paraganglioma as a diagnosis and guiding the perioperative management upon surgical treatment. The management of these unique cases has yet to be well-documented.
Patient concerns: A 14-year-old boy presented with a 5-month history of continuous and progressive elevated blood pressure and back pain. The patient, who had been diagnosed of malignant paraganglioma in the left posterior mediastinum for 3 months, received surgical resection of paraganglioma in the left posterior mediastinum, which had involved the left intervertebral foramen of T4. However, the tumor was not completely resected during the first operation.
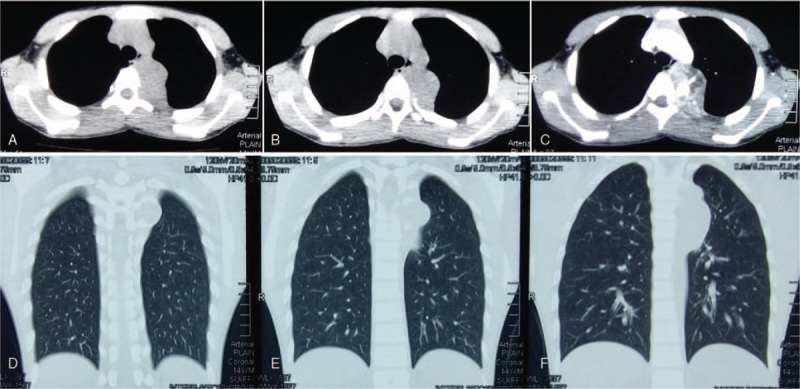
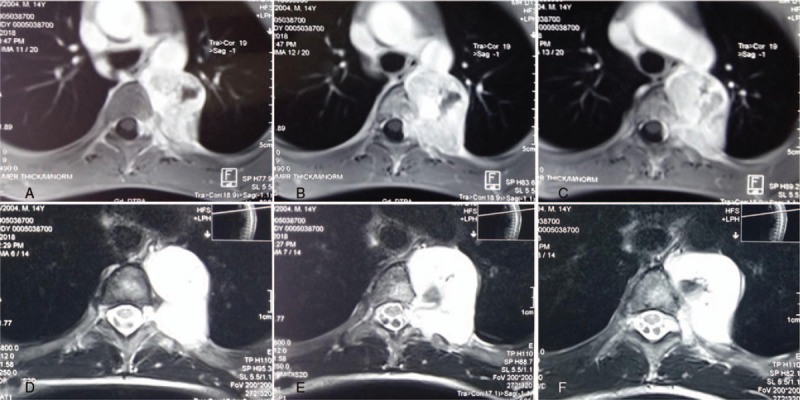
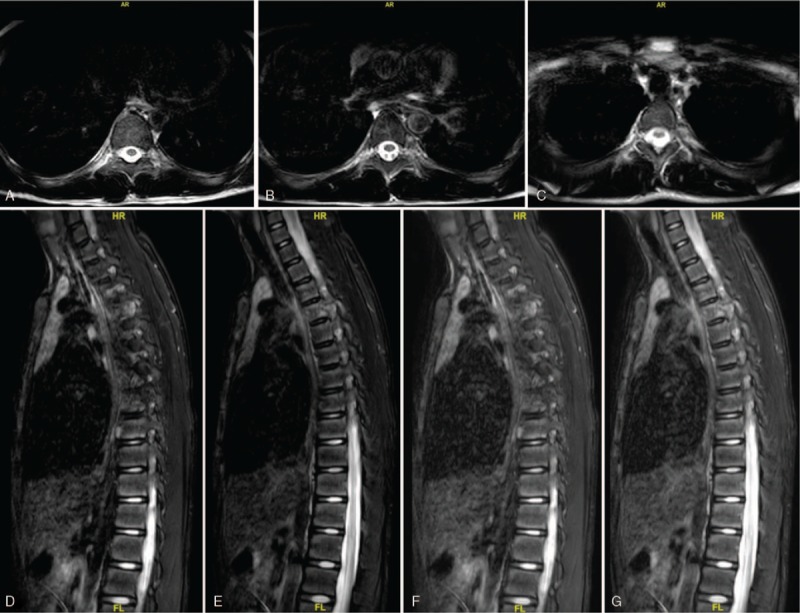
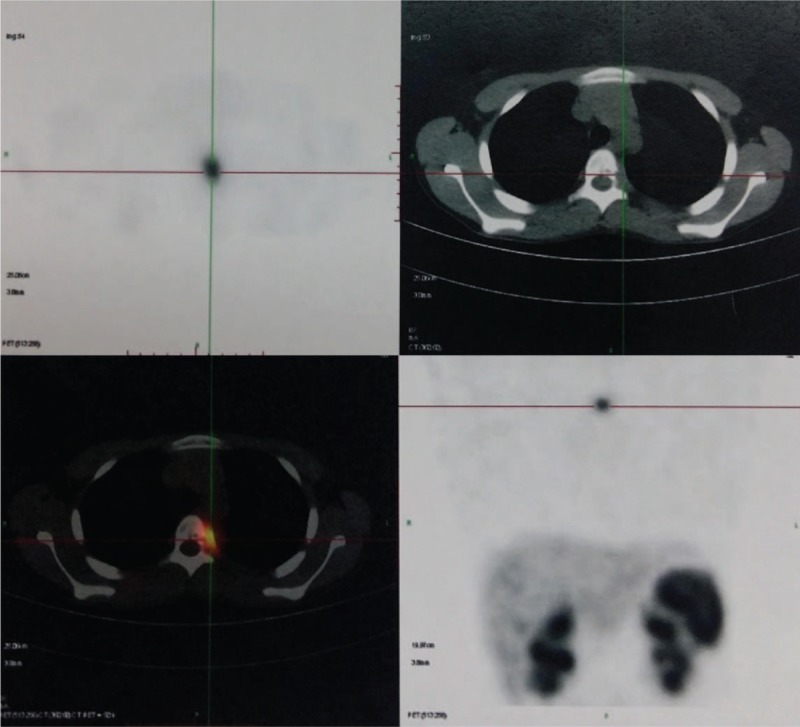
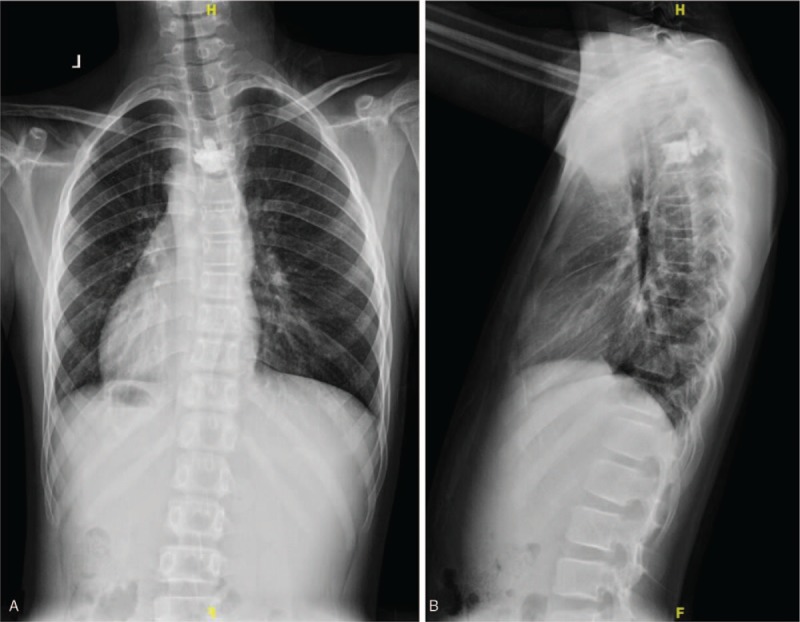
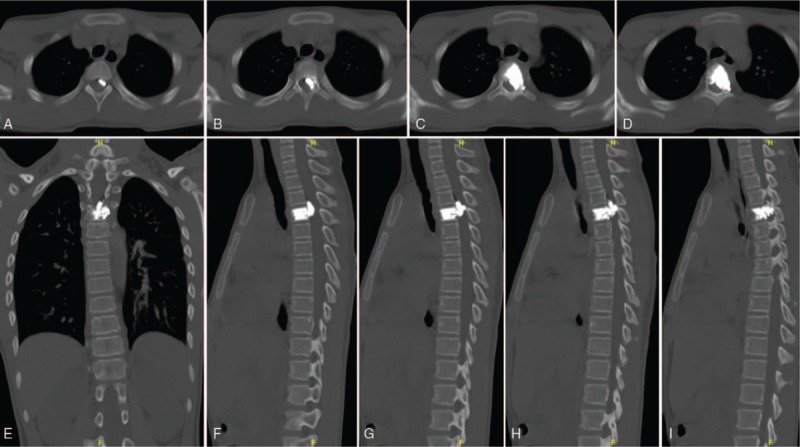
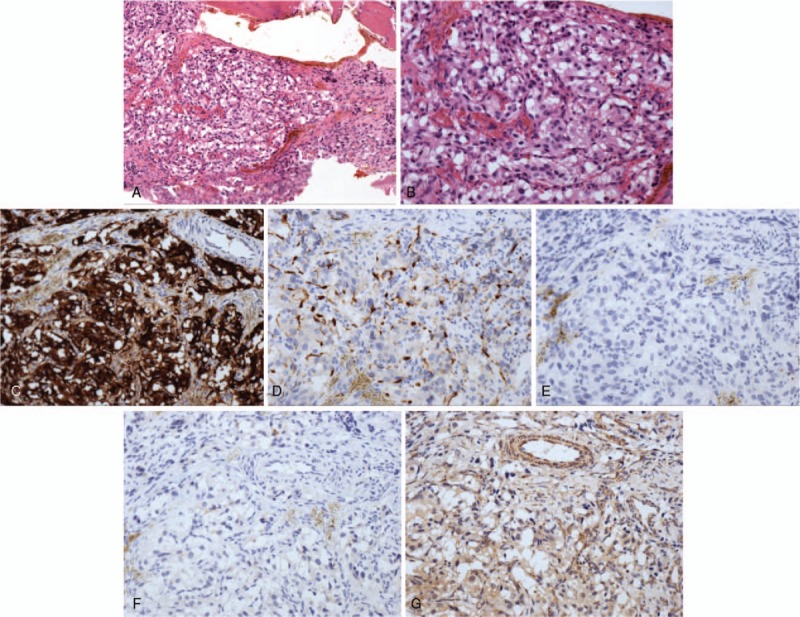
Diagnoses: Magnetic resonance imaging of spine and positron emission tomography-computed tomography showed spinal cord compression secondary to the epidural component of the T4 mass, with increased marrow infiltration of the left T4 intervertebral foramen, which was difficult to be removed. Postoperative pathology confirmed the diagnosis of spinal involvement of malignant paraganglioma.
Interventions: The patient underwent biopsy and percutaneous vertebroplasty of T4 and paravertebral lesions, and needle-track cement augmentation via a posterior approach.
Outcomes: The patient's neurological deficits improved significantly after the surgery, and the postoperative period was uneventful at the 10-month follow-up visit. There were no other complications associated with the operation during the follow-up period.
Lessons: Combined efforts of specialists from orthopedics, neurosurgery, thoracic surgery, and medical oncology led to the successful diagnosis and management of this patient. Malignant paraganglioma of thoracic spine, although rare, should be part of the differential diagnosis when the patient has a history of paraganglioma and presents with back pain and radiculopathy. We recommend the posterior approach for spinal decompression of the malignant paraganglioma when the tumor has caused neurological deficits. Osteoplasty by cement augmentation is also a good choice for surgical treatment. However, we need to take the potential risk of complications in bone cement applications into full consideration.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
Similar articles
-
Surgical treatment of giant chordoma in the thoracic spine combining thoracoscopic and posterior spinal surgery: A case report.Medicine (Baltimore). 2019 Aug;98(35):e16990. doi: 10.1097/MD.0000000000016990. Medicine (Baltimore). 2019. PMID: 31464948 Free PMC article.
-
Surgical management of spinal metastases of thymic carcinoma: A case report and literature review.Medicine (Baltimore). 2019 Jan;98(3):e14198. doi: 10.1097/MD.0000000000014198. Medicine (Baltimore). 2019. PMID: 30653174 Free PMC article. Review.
-
Surgical treatment of chondrosarcoma of the sacrum with cement augmentation: A case report.Medicine (Baltimore). 2019 Dec;98(50):e18413. doi: 10.1097/MD.0000000000018413. Medicine (Baltimore). 2019. PMID: 31852164 Free PMC article.
-
Management of giant benign fibrous histiocytoma in the spinal region with pleural involvement: A case report.Medicine (Baltimore). 2019 Sep;98(39):e17144. doi: 10.1097/MD.0000000000017144. Medicine (Baltimore). 2019. PMID: 31574815 Free PMC article.
-
Successful treatment of metastatic adrenocortical carcinoma in the spine: A case report and literature review.Medicine (Baltimore). 2019 Dec;98(49):e18259. doi: 10.1097/MD.0000000000018259. Medicine (Baltimore). 2019. PMID: 31804360 Free PMC article. Review.
Cited by
-
Nonfunctional extradural thoracic spine paraganglioma in a pediatric patient: a case report.J Surg Case Rep. 2020 Aug 24;2020(8):rjaa190. doi: 10.1093/jscr/rjaa190. eCollection 2020 Aug. J Surg Case Rep. 2020. PMID: 32855790 Free PMC article.
References
-
- Jia Q, Yin H, Yang J, et al. Treatment and outcome of metastatic paraganglioma of the spine. Eur Spine J 2018;27:859–67. - PubMed
-
- Yin M, Huan Q, Sun Z, et al. Clinical characteristics and surgical treatment of spinal paraganglioma: a case series of 18patients. Clin Neurol Neurosurg 2017;158:20–6. - PubMed
-
- Dillard-Cannon E, Atsina KB, Ghobrial G, et al. Lumbar paraganglioma. J Clin Neurosci 2016;30:149–51. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
