

Plasma Metabolic Signature and Abnormalities in HIV-Infected Individuals on Long-Term Successful Antiretroviral Therapy
- PMID: 31574898
- PMCID: PMC6835959
- DOI: 10.3390/metabo9100210
Plasma Metabolic Signature and Abnormalities in HIV-Infected Individuals on Long-Term Successful Antiretroviral Therapy
Abstract
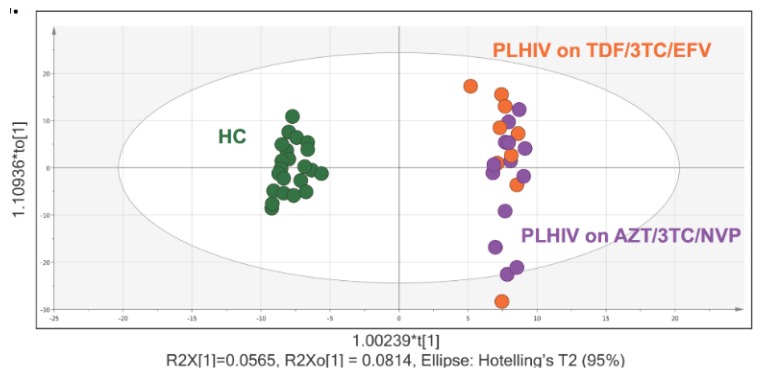
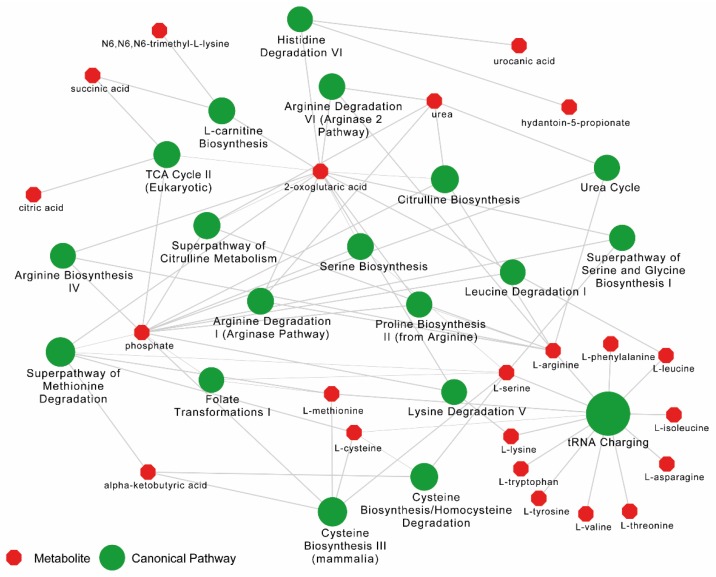
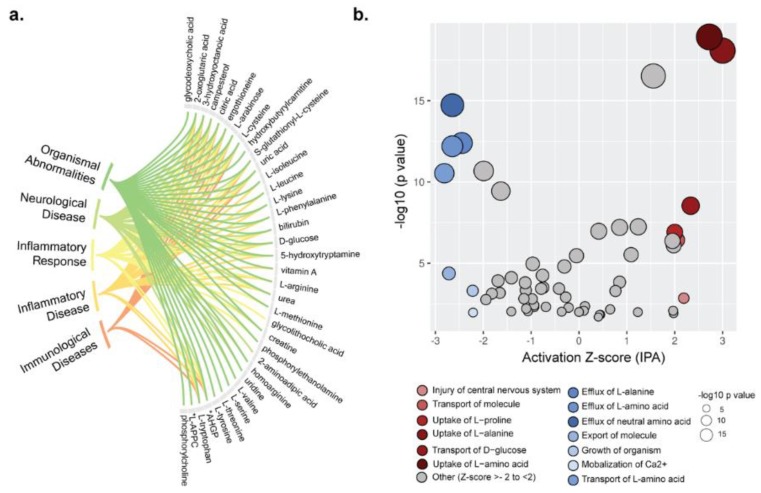
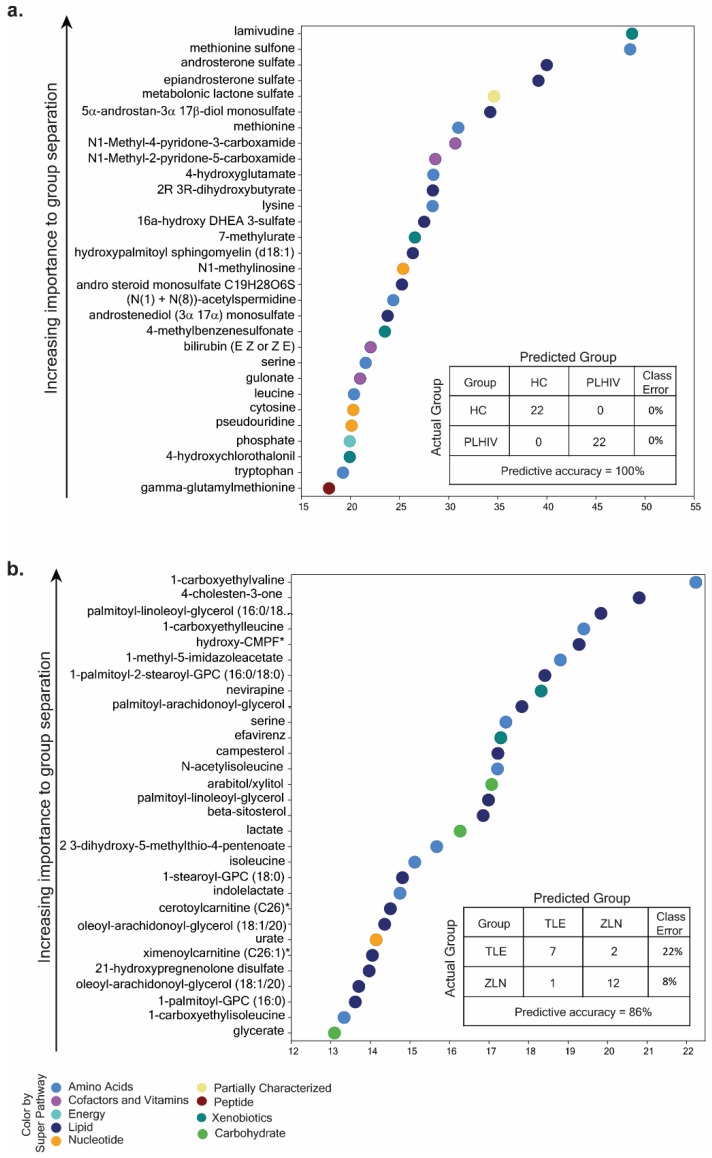
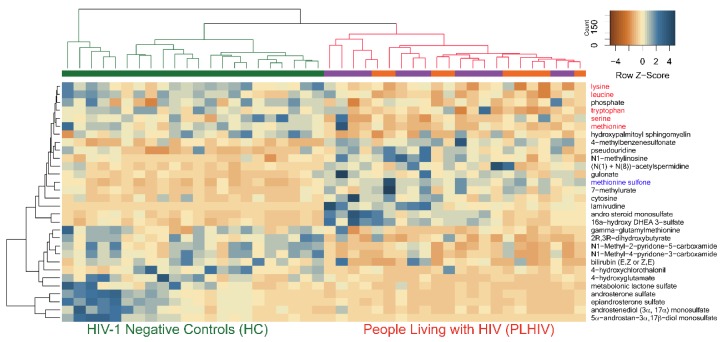
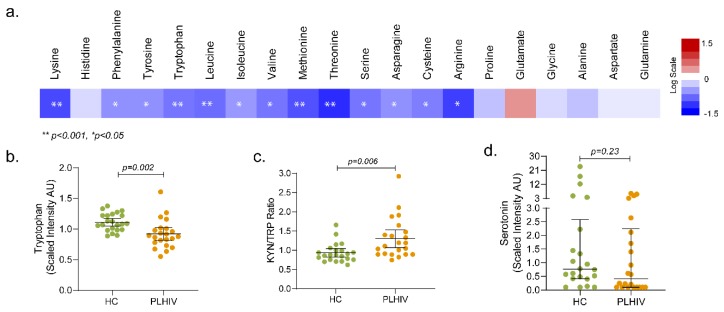
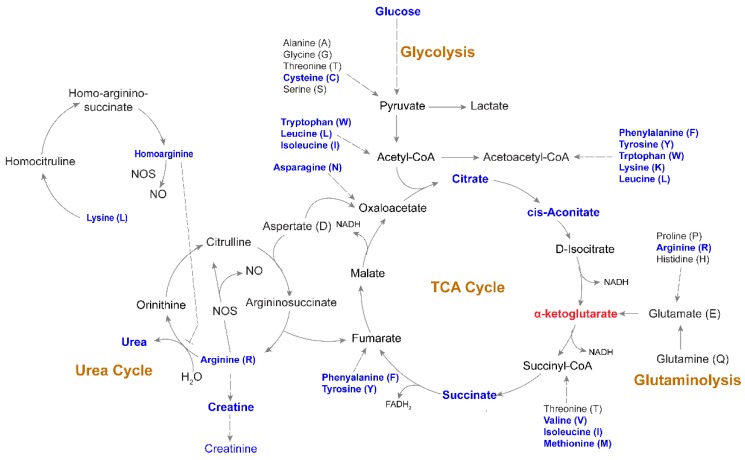
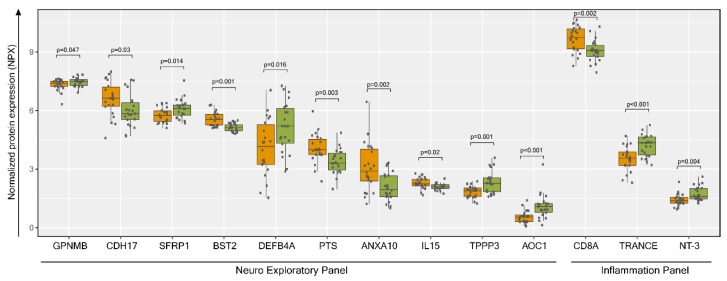
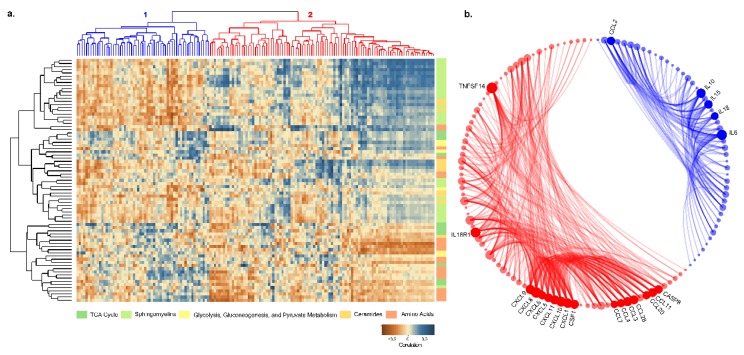
Targeted metabolomics studies reported metabolic abnormalities in both treated and untreated people living with human immunodeficiency virus (HIV) (PLHIV). The present study aimed to understand the plasma metabolomic changes and predicted the risk of accelerated aging in PLHIV on long-term suppressive antiretroviral therapy (ART) in a case-control study setting and its association with the plasma proteomics biomarkers of inflammation and neurological defects. Plasma samples were obtained from PLHIV on successful long-term ART for more than five years (n = 22) and matched HIV-negative healthy individuals (n = 22, HC herein). Untargeted metabolite profiling was carried out using ultra-high-performance liquid chromatography/mass spectrometry/mass spectrometry (UHPLC/MS/MS). Plasma proteomics profiling was performed using proximity extension assay targeting 184 plasma proteins. A total of 250 metabolites differed significantly (p < 0.05, q < 0.1) between PLHIV and HC. Plasma levels of several essential amino acids except for histidine, branched-chain amino acids, and aromatic amino acids (phenylalanine, tyrosine, tryptophan) were significantly lower in PLHIV compared to HC. Machine-learning prediction of metabolite changes indicated a higher risk of inflammatory and neurological diseases in PLHIV. Metabolic abnormalities were observed in amino-acid levels, energetics, and phospholipids and complex lipids, which may reflect known differences in lipoprotein levels in PLHIV that can resemble metabolic syndrome (MetS).
Keywords: HIV/acquired immune deficiency syndrome (AIDS); antiretroviral therapy; targeted proteomics; untargeted metabolomics.
Conflict of interest statement
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Scarpellini B., Zanoni M., Sucupira M.C., Truong H.M., Janini L.M., Segurado I.D., Diaz R.S. Plasma Metabolomics Biosignature According to HIV Stage of Infection, Pace of Disease Progression, Viremia Level and Immunological Response to Treatment. PLoS ONE. 2016;11:e0161920. doi: 10.1371/journal.pone.0161920. - DOI - PMC - PubMed
-
- Siegel M.O., Borkowska A.G., Dubrovsky L., Roth M., Welti R., Roberts A.D., Parenti D.M., Simon G.L., Sviridov D., Simmens S., et al. HIV infection induces structural and functional changes in high density lipoproteins. Atherosclerosis. 2015;243:19–29. doi: 10.1016/j.atherosclerosis.2015.08.036. - DOI - PMC - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
