

Prevalence and impact of risk factors for poor asthma outcomes in a large, specialist-managed patient cohort: a real-life study
- PMID: 31576150
- PMCID: PMC6768014
- DOI: 10.2147/JAA.S211246
Prevalence and impact of risk factors for poor asthma outcomes in a large, specialist-managed patient cohort: a real-life study
Abstract
Background: Risk factors for poor asthma outcomes may have considerable influence on the control level and medical care of asthmatic patients. Our objective was to conduct a study that provides data on the level of symptom control and the frequency of specific risk factors for poor asthma outcomes on a large patient cohort.
Methods: A cross-sectional, non-interventional real-life study was conducted among asthmatic patients treated by respiratory specialists in Hungary. Asthma control and risk factor assessment were done according to Global Initiative for Asthma guideline (Box 2-2). In the data analysis, phase descriptive statistics, graphical outputs, and Fisher's exact tests were used.
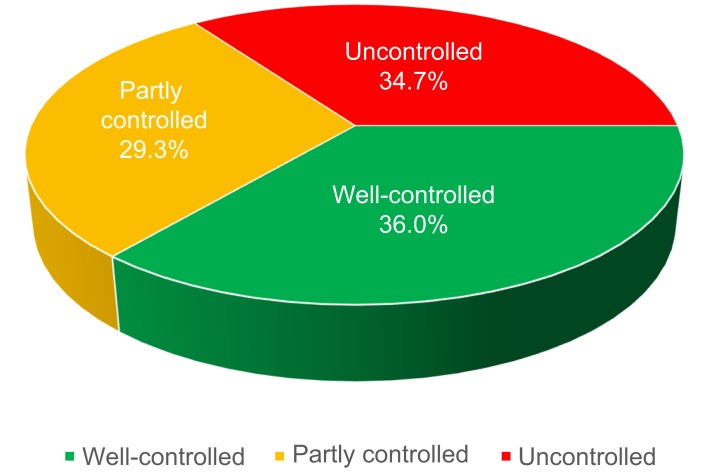
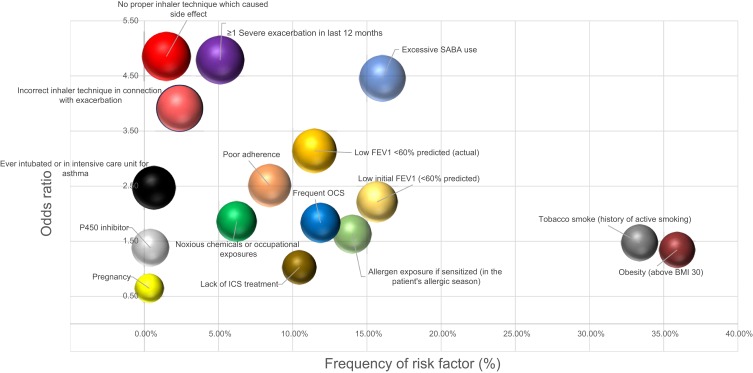
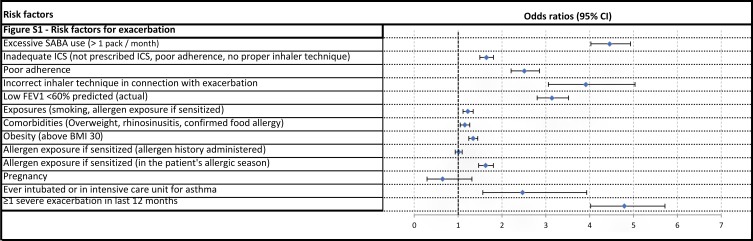
Results: Of 12743 patients enrolled by 187 specialists, asthma was well controlled in 36.0%, partially controlled in 29.29%, and uncontrolled in 34.71% of the cases. The most common comorbidities were rhinitis/sinusitis (66.84%), cardiovascular diseases (43.81%), and gastroesophageal reflux disease (20.11%). The following risk factors had the strongest relationship with uncontrolled disease: incorrect inhaler technique causing side effects (odds ratio, OR 4.86, 3.51-6.8), previous severe exacerbation (OR 4.79, 4.02-5.72), high short-acting beta agonist (SABA) use (OR 4.46, 4.03-4.93), incorrect inhaler technique associated with an exacerbation (OR 3.91, 3.06-5.03), and persistently low forced expiratory volume in 1 s (FEV1, OR 3.14, 2.8-3.52). The most frequent risk factors were smoking (OR 1.47, 1.36-1.59) and obesity (OR 1.34, 1.24-1.45). Furthermore, high loss of control was associated with an initial low FEV1 (OR 2.21, 2.01-2.44), frequent oral corticosteroid (OCS) use (OR 1.83, 1.64-2.05), poor adherence to treatment (OR 2.51, 2.21-2.86), and allergen exposure (OR 1.63, 1.47-1.81).
Conclusions: This study indicated that the presence of risk factors for poor asthma outcomes listed by the Global Initiative for Asthma document significantly influenced actual control level in a real-world large patient cohort, with high SABA use, previous severe exacerbation, incorrect inhaler technique, persistently low FEV1, and poor adherence to treatment having the highest impact.
Keywords: asthma; comorbidity; exacerbation; poor outcomes; reliever use; risk factors.
© 2019 Tomisa et al.
Conflict of interest statement
VM, LT, and ZS had consultant arrangements with AstraZeneca, Berlin-Chemie, Boehringer Ingelheim, Chiesi, GSK, Novartis, Orion, TEVA, and Takeda. GT and AH are employees of Chiesi Hungary Ltd. VM reports personal fees from GSK, AstraZeneca, Berlin Chemie, Chiesi, Boehringer Ingelheim, Novartis, Orion, and TEVA, including non-financial support from Takeda, outside the submitted work. The authors report no other conflicts of interest in this work.
Figures


References
-
- World Health Organisation. Global surveillance, prevention and control of chronic respiratory diseases: a comprehensive approach; 2007. Available from: http://www.who.int/respiratory/publications/global_surveillance/en/. Accessed October16, 2018.
-
- Soriano JB, Abajobir AA, Abate KH, et al. Global, regional, and national deaths, prevalence, disability-adjusted life years, and years lived with disability for chronic obstructive pulmonary disease and asthma, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet Respir Med. 2017;5(9):691–706. doi:10.1016/S2213-2600(17)30234-5 - DOI - PMC - PubMed
-
- Global Initiative for Asthma. Global strategy for asthma management and prevention; 2018. Available from:https://ginasthma.org/2018-gina-report-global-strategy-for-asthma-manage.... Accessed 16October 2018.
LinkOut - more resources
Full Text Sources
