

Effect of open-lung vs conventional perioperative ventilation strategies on postoperative pulmonary complications after on-pump cardiac surgery: the PROVECS randomized clinical trial
- PMID: 31576435
- PMCID: PMC9889189
- DOI: 10.1007/s00134-019-05741-8
Effect of open-lung vs conventional perioperative ventilation strategies on postoperative pulmonary complications after on-pump cardiac surgery: the PROVECS randomized clinical trial
Abstract
Purpose: To evaluate whether a perioperative open-lung ventilation strategy prevents postoperative pulmonary complications after elective on-pump cardiac surgery.
Methods: In a pragmatic, randomized, multicenter, controlled trial, we assigned patients planned for on-pump cardiac surgery to either a conventional ventilation strategy with no ventilation during cardiopulmonary bypass (CPB) and lower perioperative positive end-expiratory pressure (PEEP) levels (2 cm H2O) or an open-lung ventilation strategy that included maintaining ventilation during CPB along with perioperative recruitment maneuvers and higher PEEP levels (8 cm H2O). All study patients were ventilated with low-tidal volumes before and after CPB (6 to 8 ml/kg of predicted body weight). The primary end point was a composite of pulmonary complications occurring within the first 7 postoperative days.
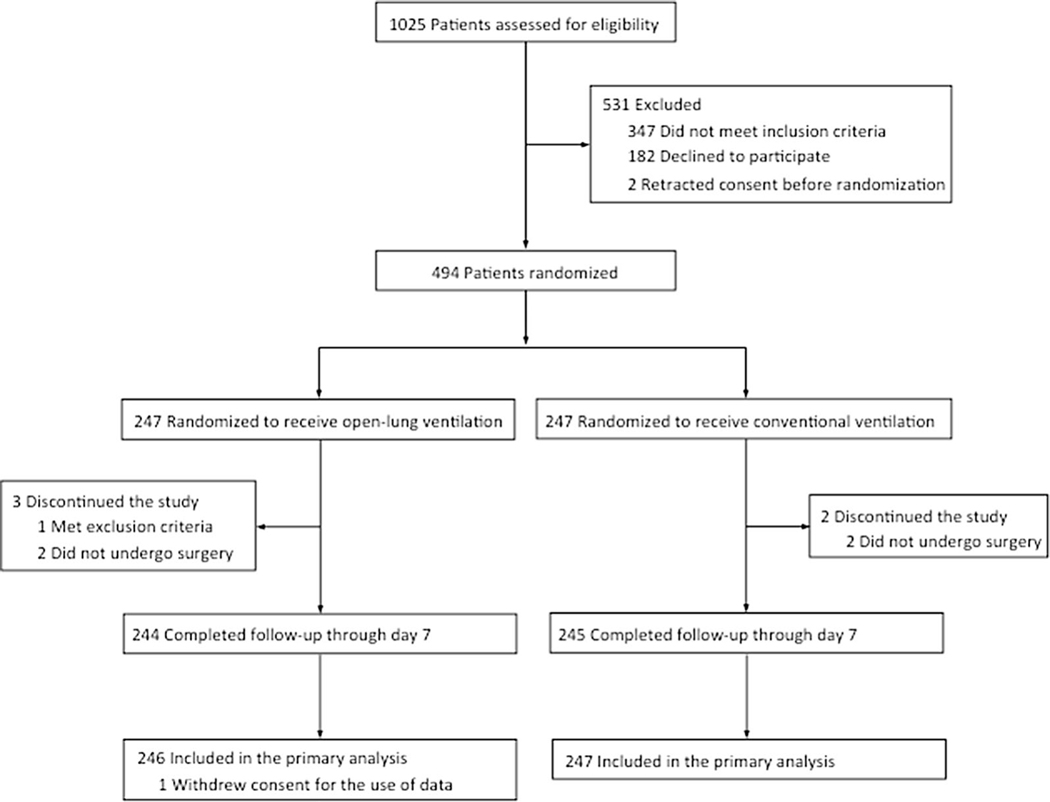
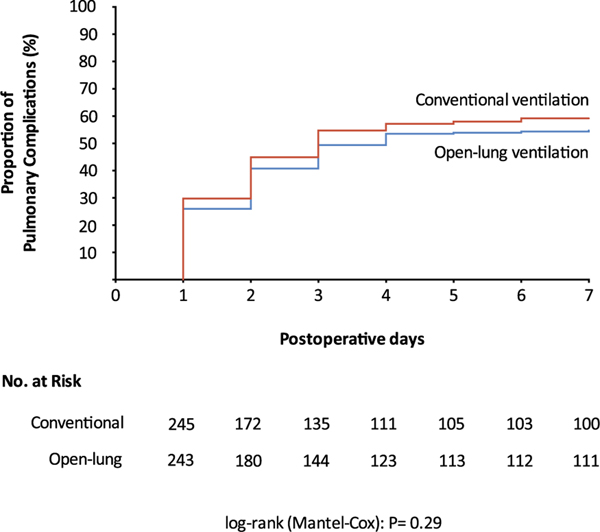
Results: Among 493 randomized patients, 488 completed the study (mean age, 65.7 years; 360 (73.7%) men; 230 (47.1%) underwent isolated valve surgery). Postoperative pulmonary complications occurred in 133 of 243 patients (54.7%) assigned to open-lung ventilation and in 145 of 245 patients (59.2%) assigned to conventional ventilation (p = 0.32). Open-lung ventilation did not significantly reduce the use of high-flow nasal oxygenotherapy (8.6% vs 9.4%; p = 0.77), non-invasive ventilation (13.2% vs 15.5%; p = 0.46) or new invasive mechanical ventilation (0.8% vs 2.4%, p = 0.28). Mean alive ICU-free days at postoperative day 7 was 4.4 ± 1.3 days in the open-lung group vs 4.3 ± 1.3 days in the conventional group (mean difference, 0.1 ± 0.1 day, p = 0.51). Extra-pulmonary complications and adverse events did not significantly differ between groups.
Conclusions: A perioperative open-lung ventilation including ventilation during CPB does not reduce the incidence of postoperative pulmonary complications as compared with usual care. This finding does not support the use of such a strategy in patients undergoing on-pump cardiac surgery.
Trial registration: Clinicaltrials.gov Identifier: NCT02866578. https://clinicaltrials.gov/ct2/show/NCT02866578.
Keywords: Cardiac surgery; Cardiopulmonary bypass; Open-lung ventilation; PEEP; Postoperative pulmonary complications; Recruitment maneuvers.
Figures
References
-
- Milot J, Perron J, Lacasse Y, Letourneau L, Cartier PC, Maltais F (2001) Incidence and predictors of ARDS after cardiac surgery. Chest 119:884–888 - PubMed
-
- Ng CS, Wan S, Yim AP, Arifi AA (2002) Pulmonary dysfunction after cardiac surgery. Chest 121:1269–1277 - PubMed
-
- Stephan F, Barrucand B, Petit P, Rezaiguia-Delclaux S, Medard A, Delannoy B, Cosserant B, Flicoteaux G, Imbert A, Pilorge C, Berard L, Bi POPSG (2015) High-flow nasal oxygen vs noninvasive positive airway pressure in hypoxemic patients after cardiothoracic surgery: a randomized clinical trial. JAMA 313:2331–2339 - PubMed
-
- Serpa Neto A, Hemmes SN, Barbas CS, Beiderlinden M, FernandezBustamante A, Futier E, Hollmann MW, Jaber S, Kozian A, Licker M, Lin WQ, Moine P, Scavonetto F, Schilling T, Selmo G, Severgnini P, Sprung J, Treschan T, Unzueta C, Weingarten TN, Wolthuis EK, Wrigge H, Gama de Abreu M, Pelosi P, Schultz MJ, investigators PN (2014) Incidence of mortality and morbidity related to postoperative lung injury in patients who have undergone abdominal or thoracic surgery: a systematic review and meta-analysis. Lancet Respir Med 2:1007–1015 - PubMed
