

Diabetic kidney disease: new clinical and therapeutic issues. Joint position statement of the Italian Diabetes Society and the Italian Society of Nephrology on "The natural history of diabetic kidney disease and treatment of hyperglycemia in patients with type 2 diabetes and impaired renal function"
- PMID: 31576500
- PMCID: PMC7007429
- DOI: 10.1007/s40620-019-00650-x
Diabetic kidney disease: new clinical and therapeutic issues. Joint position statement of the Italian Diabetes Society and the Italian Society of Nephrology on "The natural history of diabetic kidney disease and treatment of hyperglycemia in patients with type 2 diabetes and impaired renal function"
Abstract
Aims: This joint document of the Italian Diabetes Society and the Italian Society of Nephrology reviews the natural history of diabetic kidney disease (DKD) in the light of the recent epidemiological literature and provides updated recommendations on anti-hyperglycemic treatment with non-insulin agents.
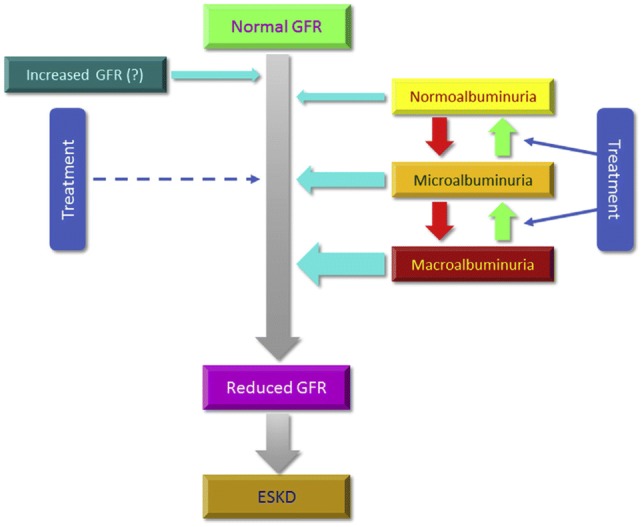
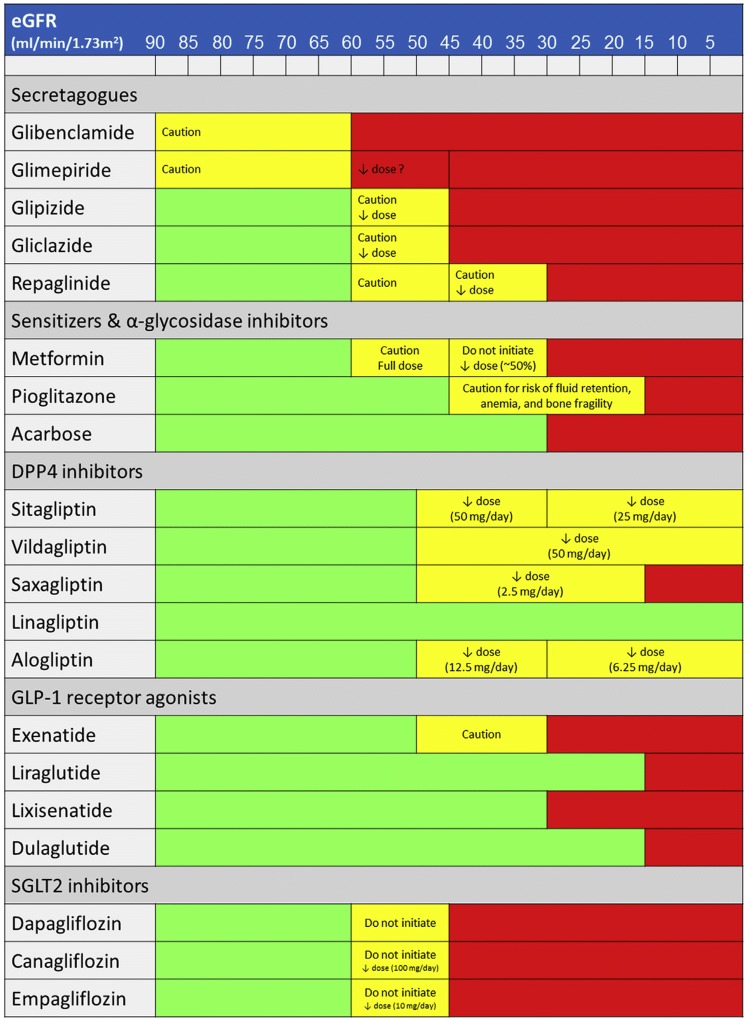
Data synthesis: Recent epidemiological studies have disclosed a wide heterogeneity of DKD. In addition to the classical albuminuric phenotype, two new albuminuria-independent phenotypes have emerged, i.e., "nonalbuminuric renal impairment" and "progressive renal decline", suggesting that DKD progression toward end-stage kidney disease (ESKD) may occur through two distinct pathways, albuminuric and nonalbuminuric. Several biomarkers have been associated with decline of estimated glomerular filtration rate (eGFR) independent of albuminuria and other clinical variables, thus possibly improving ESKD prediction. However, the pathogenesis and anatomical correlates of these phenotypes are still unclear. Also the management of hyperglycemia in patients with type 2 diabetes and impaired renal function has profoundly changed during the last two decades. New anti-hyperglycemic drugs, which do not cause hypoglycemia and weight gain and, in some cases, seem to provide cardiorenal protection, have become available for treatment of these individuals. In addition, the lowest eGFR safety thresholds for some of the old agents, particularly metformin and insulin secretagogues, have been reconsidered.
Conclusions: The heterogeneity in the clinical presentation and course of DKD has important implications for the diagnosis, prognosis, and possibly treatment of this complication. The therapeutic options for patients with type 2 diabetes and impaired renal function have substantially increased, thus allowing a better management of these individuals.
Keywords: Albuminuria; Anti-hyperglycemic therapy; Diabetes mellitus; Diabetic nephropathy; End-stage kidney disease; Estimated glomerular filtration rate.
Conflict of interest statement
GPu reported lecture and/or consultant fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, MundiPharma, Novartis, Novo Nordisk, Sigma-Tau, Takeda, and travel grants from AstraZeneca, Laboratori Guidotti, Sanofi, and Takeda. GPe reported lecture fees from AstraZeneca, Boehringer Ingelheim, Eli Lilly, Merck Sharp & Dohme, Novo Nordisk, Sigma-Tau and Takeda and travel grants from AstraZeneca, Novo Nordisk and Takeda. AN reported consultant and/or lecture fees from Amgen, AstraZeneca, Boehringer Ingelheim, Eli Lilly and research grants from Boehringer Ingelheim, Eli Lilly. LDN reported lecture and/or consultant fees from Astellas, AstraZeneca, Eli Lilly, MundiPharma, Janssen, Vifor Fresenius. No other disclosures were reported.
Figures
References
-
- Ritz E, Zeng XX, Rychlík I. Clinical manifestation and natural history of diabetic nephropathy. Contrib Nephrol. 2011;170:19–27. - PubMed
-
- Pugliese G. Updating the natural history of diabetic nephropathy. Acta Diabetol. 2014;51:905–915. - PubMed
-
- American Diabetes Association Standards of medical care in diabetes—2018. Diabetes Care. 2018;41(Suppl 1):S1–S159.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
