

A phase 1/2a, dose-escalation, safety and preliminary efficacy study of oral therapeutic vaccine in subjects with cervical intraepithelial neoplasia 3
- PMID: 31576684
- PMCID: PMC6779607
- DOI: 10.3802/jgo.2019.30.e88
A phase 1/2a, dose-escalation, safety and preliminary efficacy study of oral therapeutic vaccine in subjects with cervical intraepithelial neoplasia 3
Abstract
Objective: Persistent infection of HPV increases the chance of carcinoma in situ of cervix through stages of cervical intraepithelial neoplasia (CIN) 1, 2, and 3, and finally progresses into cervical cancer. We aimed to explore the safety and efficacy of BLS-M07 which is orally administered agent expressing human papillomavirus (HPV) 16 E7 antigen on the surface of Lactobacillus casei in patients with CIN 3.
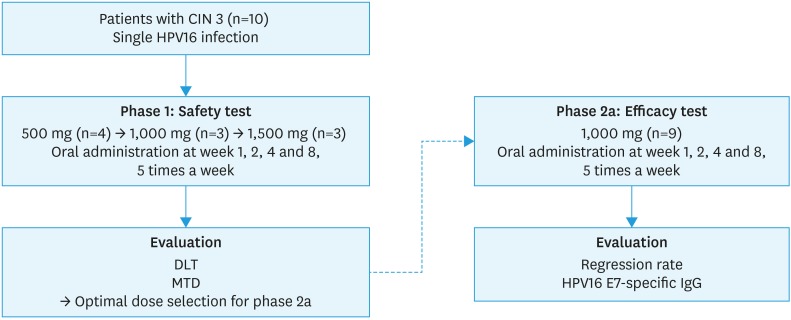
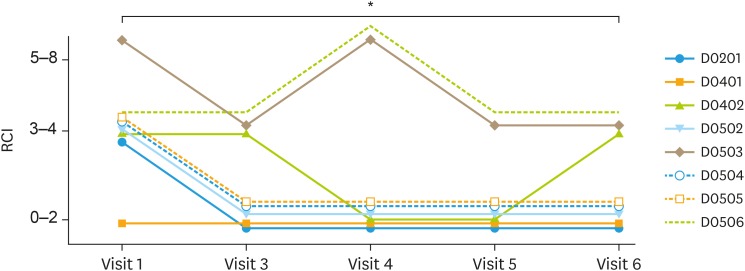
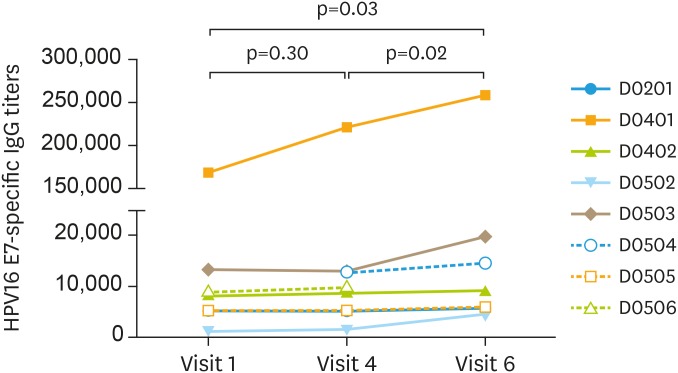
Methods: Patients with CIN 3 were recruited in our clinical trial. Reid Colposcopic Index (RCI) grading and serum HPV16 E7 specific antibody production were used to evaluate efficacy of BLS-M07. In phase 1, BLS-M07 was administered orally, 5 times a week, on weeks 1, 2, 4, and 8 with dosages of 500 mg, 1,000 mg, and 1,500 mg. In phase 2a, patients were treated with 1,000 mg. The primary endpoints were the safety and the pathologic regression on colposcopic biopsy.
Results: Nineteen patients were enrolled in the CIN 3 cohort. In phase 1, no patients experienced dose limiting toxicity. No grade 3 or 4 treatment-related adverse events or deaths were observed. At 16 weeks after treatment, RCI grading was improved and serum HPV16 E7 specific antibody production increased (p<0.05). Six of 8 (75%) patients with CIN 3 were cured in phase 2a.
Conclusions: Oral immunization with BLS-M07 increases production of serum HPV16 E7 specific antibody which induces protective humoral immunity. The safety of this oral vaccine was proved and could be a competitive non-surgical therapeutic agent of CIN 3.
Trial registration: ClinicalTrials.gov Identifier: NCT02195089.
Keywords: Cervical Intraepithelial Neoplasia; Papillomavirus E7 Proteins; Papillomavirus Vaccines.
Copyright © 2019. Asian Society of Gynecologic Oncology, Korean Society of Gynecologic Oncology.
Conflict of interest statement
Young-Chul Park, Moon-Hee Sung, Hong-Gyu Park from BioLeaders, Corp. are employees of and/or shareholders of the company, which is developing BLS-M07 vaccine. The remaining authors declare no competing financial interests.
Figures
Comment in
-
Therapeutic vaccination using HPV 16 E7 to eradicate CIN3.J Gynecol Oncol. 2019 Nov;30(6):e119. doi: 10.3802/jgo.2019.30.e119. J Gynecol Oncol. 2019. PMID: 31576704 Free PMC article. No abstract available.
-
Comments on: a phase 1/2a, dose-escalation, safety and preliminary efficacy study of oral therapeutic vaccine in subjects with cervical intraepithelial neoplasia 3.J Gynecol Oncol. 2020 Mar;31(2):e43. doi: 10.3802/jgo.2020.31.e43. J Gynecol Oncol. 2020. PMID: 32100488 Free PMC article. No abstract available.
-
In reply: the evaluation of IgG titers' stability from blood samples is necessary.J Gynecol Oncol. 2020 Mar;31(2):e44. doi: 10.3802/jgo.2020.31.e44. J Gynecol Oncol. 2020. PMID: 32100489 Free PMC article. No abstract available.
References
-
- Einstein MH, Schiller JT, Viscidi RP, Strickler HD, Coursaget P, Tan T, et al. Clinician's guide to human papillomavirus immunology: knowns and unknowns. Lancet Infect Dis. 2009;9:347–356. - PubMed
-
- Parkin DM, Bray F. Chapter 2: the burden of HPV-related cancers. Vaccine. 2006;24(Suppl 3):S3/11–25. - PubMed
-
- Cox JT. The development of cervical cancer and its precursors: what is the role of human papillomavirus infection? Curr Opin Obstet Gynecol. 2006;18(Suppl 1):s5–s13. - PubMed
-
- Dalstein V, Riethmuller D, Prétet JL, Le Bail Carval K, Sautière JL, Carbillet JP, et al. Persistence and load of high-risk HPV are predictors for development of high-grade cervical lesions: a longitudinal French cohort study. Int J Cancer. 2003;106:396–403. - PubMed
-
- Snijders PJ, Steenbergen RD, Heideman DA, Meijer CJ. HPV-mediated cervical carcinogenesis: concepts and clinical implications. J Pathol. 2006;208:152–164. - PubMed
