

Investigating the role of immunotherapy in advanced/recurrent female genital tract melanoma: a preliminary experience
- PMID: 31576688
- PMCID: PMC6779609
- DOI: 10.3802/jgo.2019.30.e94
Investigating the role of immunotherapy in advanced/recurrent female genital tract melanoma: a preliminary experience
Abstract
Objective: immunotherapy with immune checkpoint inhibitors has become one of the standard therapeutic modalities for patients with advanced melanoma. Melanoma of the female lower genital tract is a rare and aggressive disease, with poor long-term clinical outcomes. To date, no study evaluated the role of immunotherapy in metastatic melanoma of the lower genital tract.
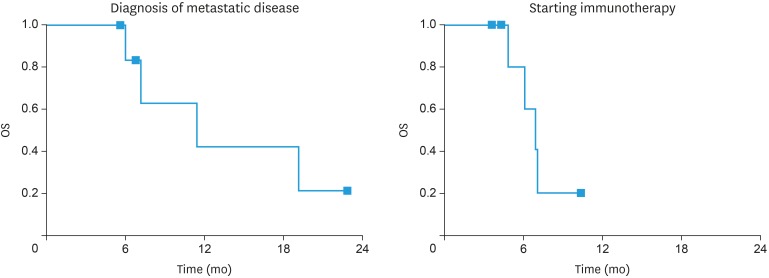
Methods: Data of women with metastatic melanoma of the lower genital tract were prospectively collected. Survival outcomes over time was assessed using Kaplan-Meier model.
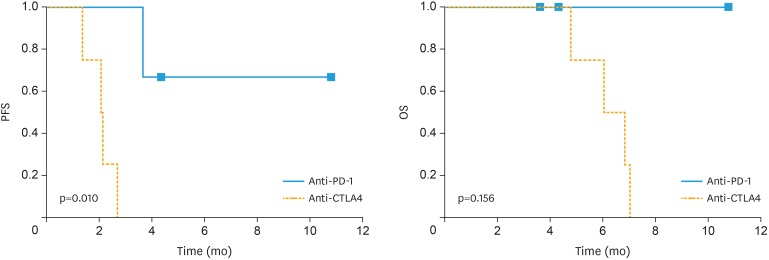
Results: Seven cases of metastatic melanoma of the lower genital tract (vulva [n=2], vagina [n=4], and uterine cervix [n=1]) treated with immune checkpoint inhibitors are reviewed. Two patients had metastatic disease at diagnosis, while 5 patients developed metastatic disease at a mean (standard deviation) time of 9.9 (±3.0) months from primary diagnosis. Four patients received an anti-cytotoxic T lymphocyte-associated antigen 4 (CTLA4) (ipilimumab) and 3 received an anti-programmed cell death 1 (PD-1) (pembrolizumab [n=2], nivolumab [n=1]) therapy. The response rate to immunotherapy was 28.5%. Patients receiving an anti-PD-1 experienced a better progression-free survival than patients treated with anti-CTLA4 (p=0.01, log-rank test). Although not reaching statistical significance, overall survival was better in patients having an anti-PD-1 therapy in comparison to anti-CTLA4 (p=0.15, log-rank test).
Conclusion: Results from our series confirm the poor prognosis of women with metastatic melanoma of the lower genital tract, thus supporting the need of exploring new treatment modalities. Further studies are warranted to improve knowledge on the role of immunotherapy in metastatic melanoma of the lower genital tract.
Keywords: CTLA-4; Genital; Gynecological; Immunotherapy; Melanoma; PD-1.
Copyright © 2019. Asian Society of Gynecologic Oncology, Korean Society of Gynecologic Oncology.
Conflict of interest statement
No potential conflict of interest relevant to this article was reported.
Figures
References
-
- Chang AE, Karnell LH, Menck HR. The National Cancer Data Base report on cutaneous and noncutaneous melanoma: a summary of 84,836 cases from the past decade. The American College of Surgeons Commission on Cancer and the American Cancer Society. Cancer. 1998;83:1664–1678. - PubMed
-
- Vaysse C, Pautier P, Filleron T, Maisongrosse V, Rodier JF, Lavoue V, et al. A large retrospective multicenter study of vaginal melanomas: implications for new management. Melanoma Res. 2013;23:138–146. - PubMed
-
- Mert I, Semaan A, Winer I, Morris RT, Ali-Fehmi R. Vulvar/vaginal melanoma: an updated surveillance epidemiology and end results database review, comparison with cutaneous melanoma and significance of racial disparities. Int J Gynecol Cancer. 2013;23:1118–1125. - PubMed
-
- Yi JH, Yi SY, Lee HR, Lee SI, Lim DH, Kim JH, et al. Dacarbazine-based chemotherapy as first-line treatment in noncutaneous metastatic melanoma: multicenter, retrospective analysis in Asia. Melanoma Res. 2011;21:223–227. - PubMed
