

Blood pressure extremes and severe IVH in preterm infants
- PMID: 31578033
- PMCID: PMC6962547
- DOI: 10.1038/s41390-019-0585-3
Blood pressure extremes and severe IVH in preterm infants
Abstract
Background: The optimal upper and lower limits of blood pressure in preterm infants are not known. Exceeding these thresholds may contribute to intraventricular hemorrhage (IVH).
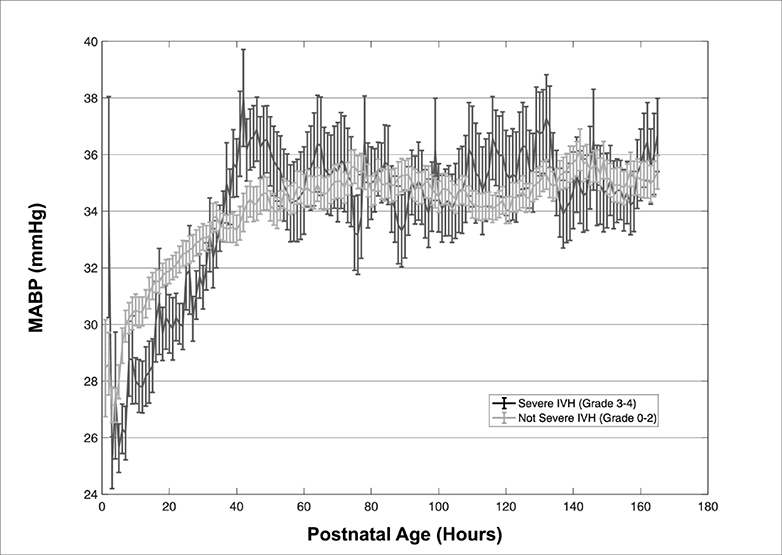
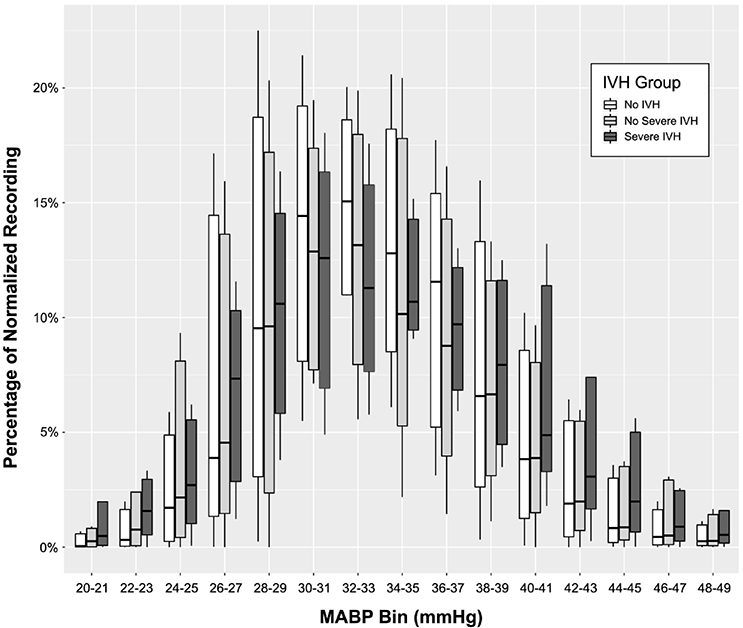
Methods: Preterm infants born ≤30 weeks GA were identified. Infants had continuous measurement of mean arterial blood pressure (MABP) for 7 days and cranial ultrasound imaging. IVH was classified as severe IVH (grade 3/4), no severe IVH (no IVH; grade 1/2), or no IVH. Mean ± SEM MABP values from hours 1-168 were calculated and sorted into bins 2 mm Hg wide. The normalized proportion of each recording spent in each bin was then calculated. Candidate limits were identified by comparison of MABP distribution in those with severe IVH vs. those without severe IVH.
Results: Eighty-five million measurements were made from 157 infants. Mean EGA was 25.2 weeks; mean BW was 749 g; 65/157 female; inotrope use in 59/157; grade 3/4 IVH in 29/157. Infants with severe IVH spent significantly more time with extreme MABP measurements (<23 mm Hg or >46 mm Hg) compared to those without severe IVH (12% vs. 8% of recording, p = 0.02).
Conclusions: Infants who developed severe IVH had substantially more unstable MABP and spent a significantly greater period of time with MABP outside of the optimal range.
Conflict of interest statement
Figures
Comment in
-
Alternative facts? Using big data to identify high and low blood pressure values.Pediatr Res. 2020 Jan;87(1):13-14. doi: 10.1038/s41390-019-0636-9. Epub 2019 Oct 25. Pediatr Res. 2020. PMID: 31652434 No abstract available.
References
-
- Volpe JJ. Neurology of the newborn. 5th ed. Philadelphia: Saunders/Elsevier; 2008.
-
- Ment LR, Oh W, Ehrenkranz RA, Philip AG, Duncan CC, Makuch RW. Antenatal steroids, delivery mode, and intraventricular hemorrhage in preterm infants. Am J Obstet Gynecol 1995;172:795–800. - PubMed
-
- Soul JS, Hammer PE, Tsuji M, et al. Fluctuating pressure-passivity is common in the cerebral circulation of sick premature infants. Pediatr Res 2007;61:467–73. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
