

Reversal of a rheologic cardiomyopathy following hematopoietic stem cell transplantation for sickle cell disease
- PMID: 31578191
- PMCID: PMC6784516
- DOI: 10.1182/bloodadvances.2019000387
Reversal of a rheologic cardiomyopathy following hematopoietic stem cell transplantation for sickle cell disease
Abstract
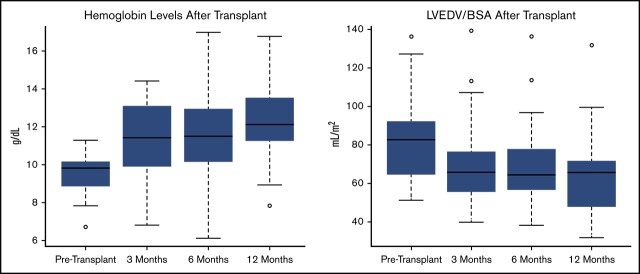
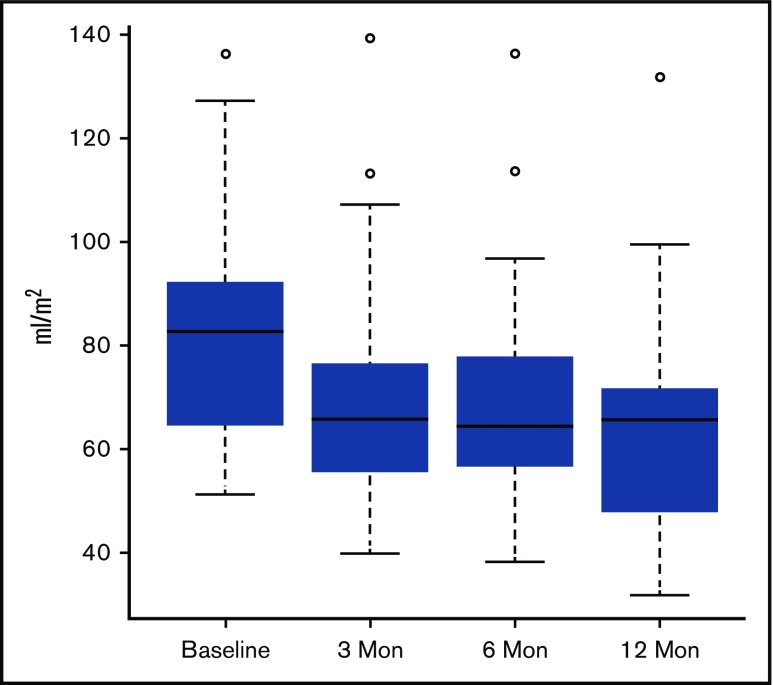
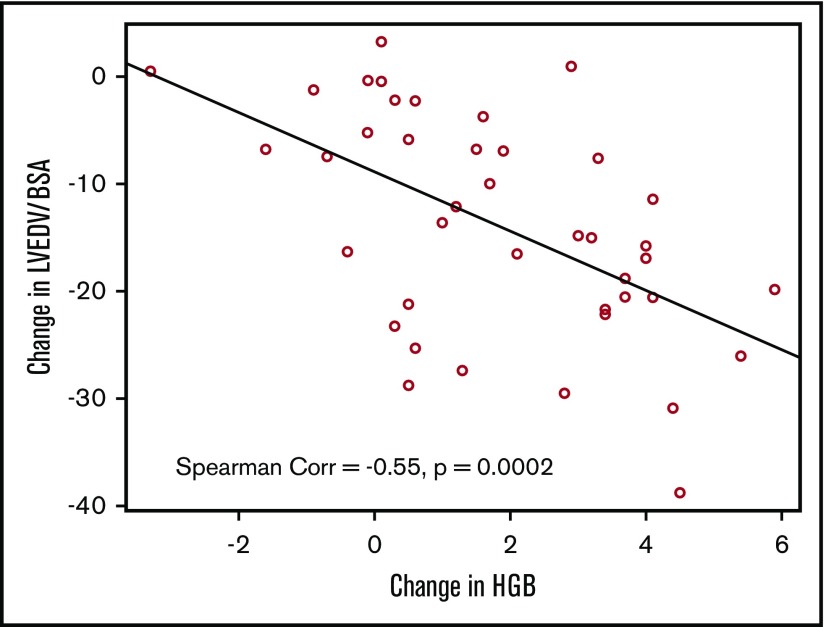
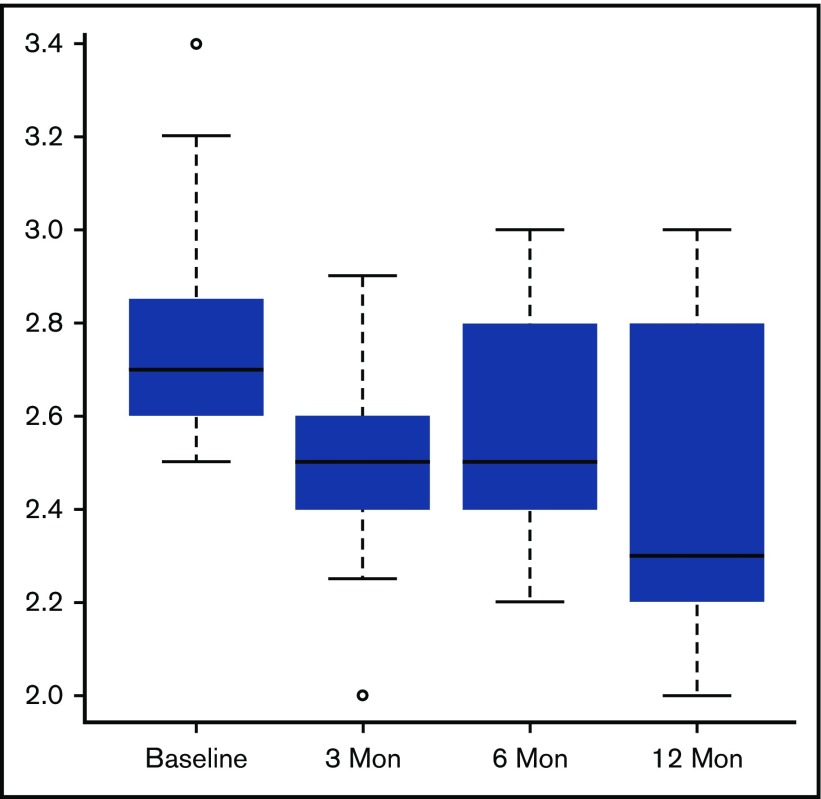
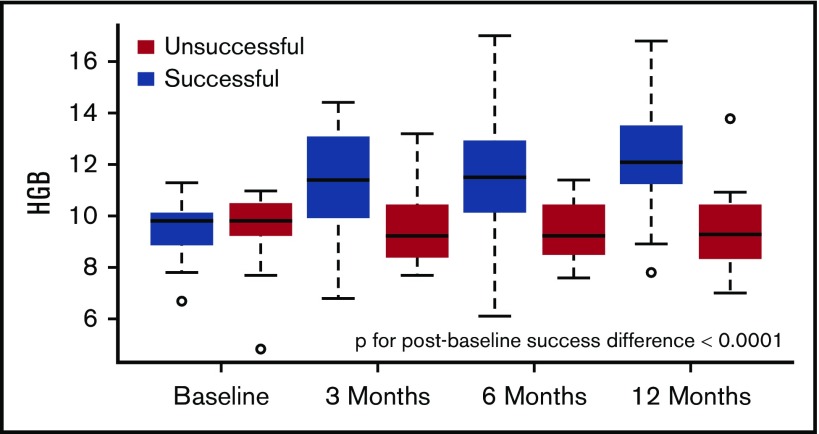
Cardiac complications have been well-described in sickle cell disease; however, it has been rare to see improvements in cardiac abnormalities following any interventions. Previous work has shown no significant structural changes after treatment with hydroxyurea. The cardiac effects of red blood cell exchange transfusion (RBCx) and hematopoietic stem cell transplantation (HSCT) have not been well described. We studied 56 patients undergoing HSCT (41 HLA-matched, 15 haploidentical), of whom 32 had RBCx within 3 months before HSCT. Echocardiograms and laboratory parameters were obtained at baseline, and at 3, 6, and 12 months following HSCT. Although hemolytic parameters and anemia improved following RBCx, there was a small increase in left ventricular volume index. Following successful HSCT, however, there were significant improvements in cardiac size, function, and diastolic filling parameters at 3 months followed by continued smaller improvements up to 1 year. There was a significant improvement in N-terminal pro B-type natriuretic peptide levels and a trend toward improvement in 6-minute walk time 1 year after HSCT. The magnitude of cardiac improvement seen following HSCT was comparable to that observed following correction of a volume overload state as seen in pregnancy or after repair of chronic valvular regurgitation. Further studies in sickle cell disease patients will help delineate which cardiac complications and what level of severity should be considered indications for HSCT.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures
References
-
- Gladwin MT. Cardiovascular complications and risk of death in sickle-cell disease. Lancet. 2016;387(10037):2565-2574. - PubMed
-
- Gladwin MT, Sachdev V, Jison ML, et al. . Pulmonary hypertension as a risk factor for death in patients with sickle cell disease. N Engl J Med. 2004;350(9):886-895. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
