

Comparison of Gait Ability of a Child with Cerebral Palsy According to the Difference of Dorsiflexion Angle of Hinged Ankle-Foot Orthosis: A Case Report
- PMID: 31578314
- PMCID: PMC6788483
- DOI: 10.12659/AJCR.916814
Comparison of Gait Ability of a Child with Cerebral Palsy According to the Difference of Dorsiflexion Angle of Hinged Ankle-Foot Orthosis: A Case Report
Abstract
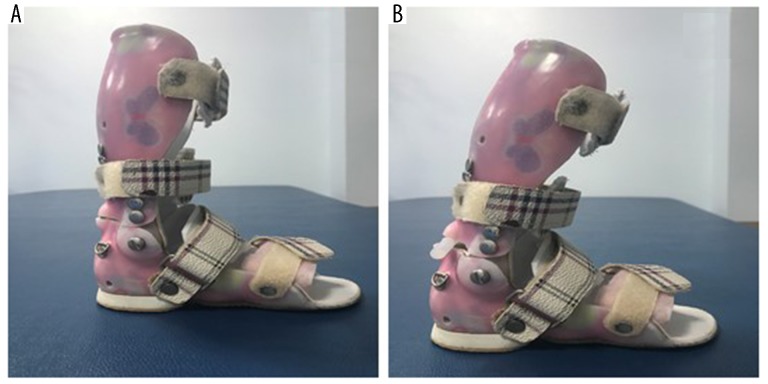
BACKGROUND The purpose of this study was to compare gait abilities in a child with spastic diplegia according to different dorsiflexion angles on hinged ankle-foot orthosis (hinged AFO). CASE REPORT This study is a case report of a child who was diagnosed with spastic diplegia and ambulated independently with the use of a hinged AFO. For gait analysis, the GAITRite® was used under 3 different conditions including barefoot, wearing regular of hinged AFO, and wearing a dorsiflexion 10° hinged AFO. The gait velocity and cadence were collected as temporal parameters, while step length, stride length, and single and double leg support time were collected as temporal spatial parameters. As a result, when a regular hinged AFO was worn on the barefoot, the gait velocity and cadence per minute were increased, whereas the step length and stride length, the single and double leg support time decreased. The gait velocity, cadence, step length, and stride length were significantly increased when dorsiflexion 10° hinged AFO was applied compared to barefoot. The gait velocity, cadence, step length, and stride length increased with dorsiflexion 10° hinged AFO compared to regular hinged AFO. CONCLUSIONS The results of this study demonstrated that wearing a dorsiflexion 10° hinged AFO would have a positive effect on improving gait ability of a child with cerebral palsy rather than wearing a bare foot and a general hinged AFO.
Conflict of interest statement
Figures
Similar articles
-
The effect of hinged ankle-foot orthoses on sit-to-stand transfer in children with spastic cerebral palsy.Arch Phys Med Rehabil. 2004 Dec;85(12):2053-7. doi: 10.1016/j.apmr.2004.05.008. Arch Phys Med Rehabil. 2004. PMID: 15605347 Clinical Trial.
-
The effect of hinged ankle-foot orthosis on gait and energy expenditure in spastic hemiplegic cerebral palsy.Disabil Rehabil. 2007 Jan 30;29(2):139-44. doi: 10.1080/17483100600876740. Disabil Rehabil. 2007. PMID: 17373095
-
The Efficacy of Ankle-Foot Orthoses on Improving the Gait of Children With Diplegic Cerebral Palsy: A Multiple Outcome Analysis.PM R. 2015 Sep;7(9):922-929. doi: 10.1016/j.pmrj.2015.03.005. Epub 2015 Mar 11. PM R. 2015. PMID: 25771349
-
Effect of ankle-foot orthoses on gait, balance and gross motor function in children with cerebral palsy: a systematic review and meta-analysis.Clin Rehabil. 2018 Sep;32(9):1175-1188. doi: 10.1177/0269215518771824. Epub 2018 May 1. Clin Rehabil. 2018. PMID: 29714066
-
Impact of Ankle-Foot Orthosis on Gait Efficiency in Ambulatory Children With Cerebral Palsy: A Systematic Review and Meta-analysis.Am J Phys Med Rehabil. 2019 Sep;98(9):759-770. doi: 10.1097/PHM.0000000000001185. Am J Phys Med Rehabil. 2019. PMID: 30920399
Cited by
-
Commonly Used Types and Recent Development of Ankle-Foot Orthosis: A Narrative Review.Healthcare (Basel). 2021 Aug 13;9(8):1046. doi: 10.3390/healthcare9081046. Healthcare (Basel). 2021. PMID: 34442183 Free PMC article. Review.
-
Passive Articulated and Non-Articulated Ankle-Foot Orthoses for Gait Rehabilitation: A Narrative Review.Healthcare (Basel). 2023 Mar 24;11(7):947. doi: 10.3390/healthcare11070947. Healthcare (Basel). 2023. PMID: 37046871 Free PMC article. Review.
-
Combination taping technique versus ankle foot orthosis on improving gait parameters in spastic cerebral palsy: A controlled randomized study.J Rehabil Med. 2021 Nov 30;53(11):jrm00240. doi: 10.2340/jrm.v53.900. J Rehabil Med. 2021. PMID: 34812472 Free PMC article. Clinical Trial.
References
-
- Scherzer AL, Tscharnuter I. Early diagnosis and therapy in cerebral palsy: A primer on infant developmental problems. 2nd ed. New York: Marcel Dekker; 1990. pp. 678–80.
-
- Krigger KW. Cerebral palsy: An overview. Am Fam Physician. 2006;73(1):91–100. - PubMed
-
- Ounpuu S, Gage JR, Davis RB. Three-dimensional lower extremity joint kinetics in normal pediatric gait. J Pediatr Orthop. 1991;11(3):341–49. - PubMed
-
- Sankar C, Mundkur N. Cerebral palsy-definition, classification, etiology and early diagnosis. Indian J Pediatr. 2005;72(10):865–68. - PubMed
-
- Middleton EA, Hurley GR, McIlwain JS. The role of rigid and hinged polypropylene ankle-foot-orthoses in the management of cerebral palsy: A case study. Prosthet Orthot Int. 1988;12(3):129–35. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
