

Technical assessment of a mobile CT scanner for image-guided brachytherapy
- PMID: 31578811
- PMCID: PMC6806478
- DOI: 10.1002/acm2.12738
Technical assessment of a mobile CT scanner for image-guided brachytherapy
Abstract
Purpose: The imaging performance and dose of a mobile CT scanner (Brainlab Airo®, Munich, Germany) is evaluated, with particular consideration to assessment of technique protocols for image-guided brachytherapy.
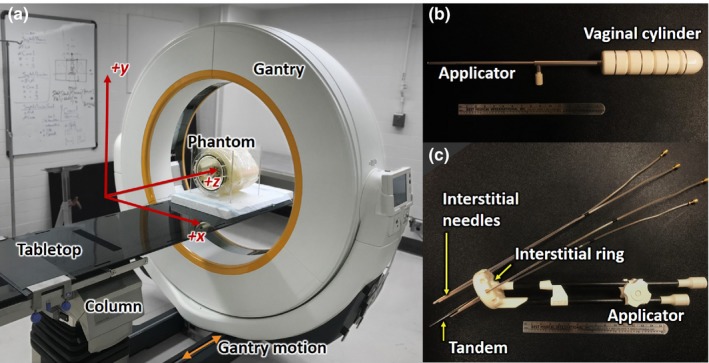
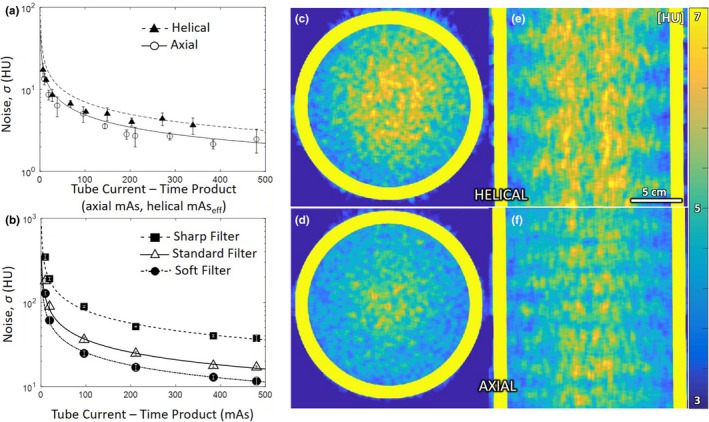
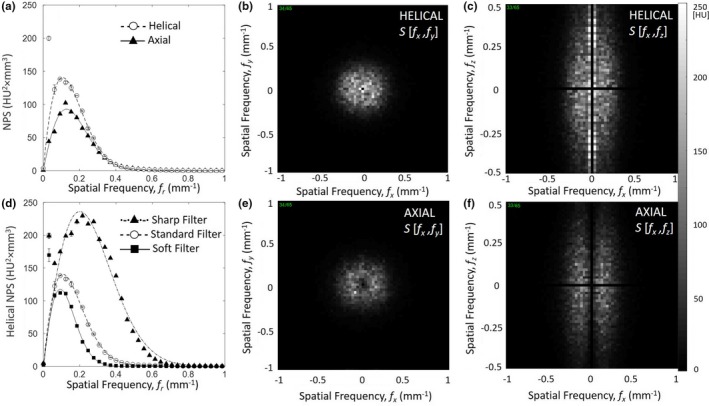
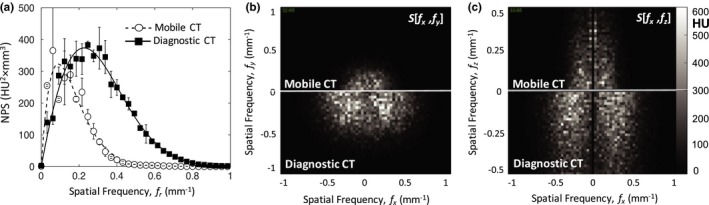
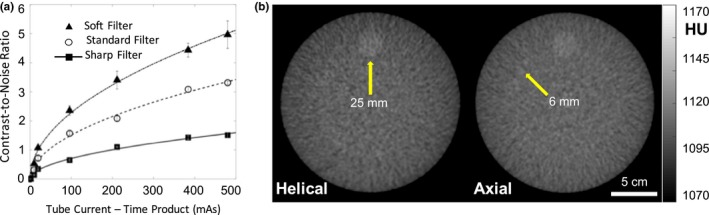
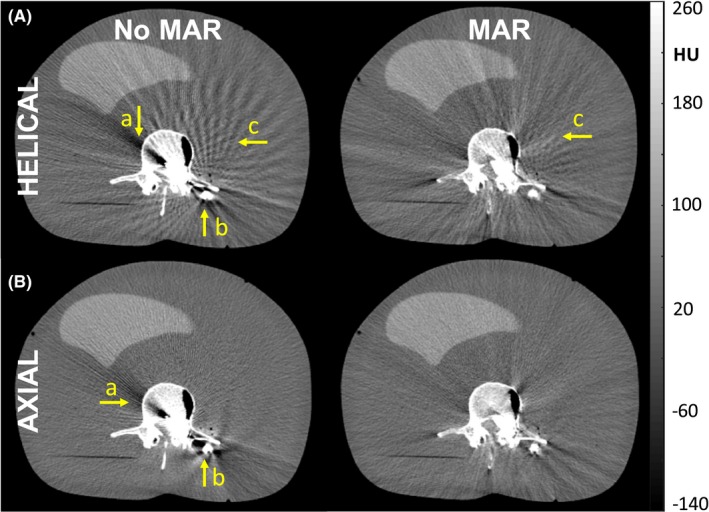
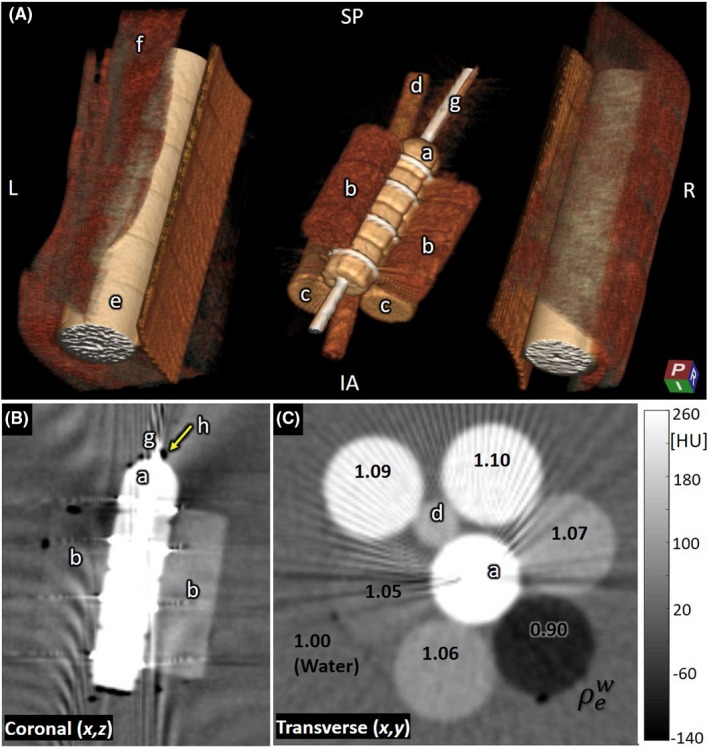
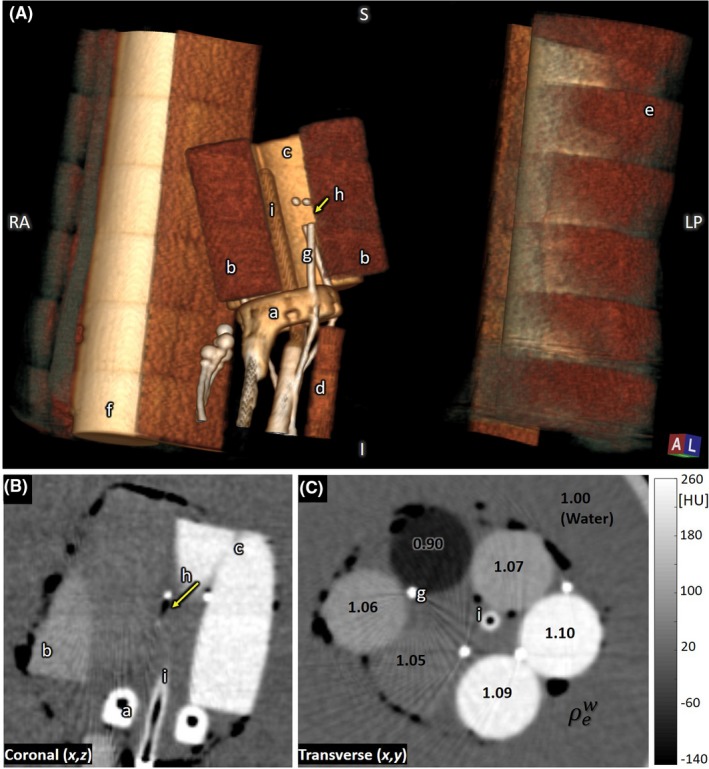
Method: Dose measurements were performed using a 100-mm-length pencil chamber at the center and periphery of 16- and 32-cm-diameter CTDI phantoms. Hounsfield unit (HU) accuracy and linearity were assessed using materials of specified electron density (Gammex RMI, Madison, WI), and image uniformity, noise, and noise-power spectrum (NPS) were evaluated in a 20-cm-diameter water phantom as well as an American College of Radiology (ACR) CT accreditation phantom (Model 464, Sun Nuclear, Melbourne, FL). Spatial resolution (modulation transfer function, MTF) was assessed with an edge-spread phantom and visually assessed with respect to line-pair patterns in the ACR phantom and in structures of interest in anthropomorphic phantoms. Images were also obtained on a diagnostic CT scanner (Big Bore CT simulator, Philips, Amsterdam, Netherlands) for qualitative and quantitative comparison. The manufacturer's metal artifact reduction (MAR) algorithm was assessed in an anthropomorphic body phantom containing surgical instrumentation. Performance in application to brachytherapy was assessed with a set of anthropomorphic brachytherapy phantoms - for example, a vaginal cylinder and interstitial ring and tandem.
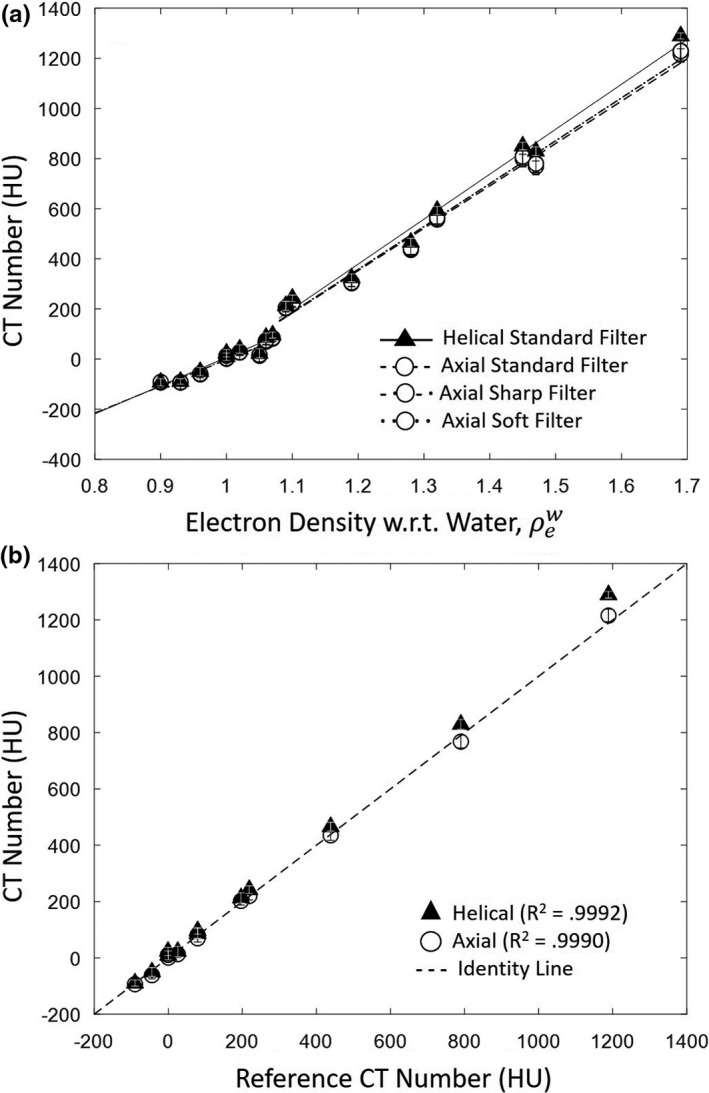
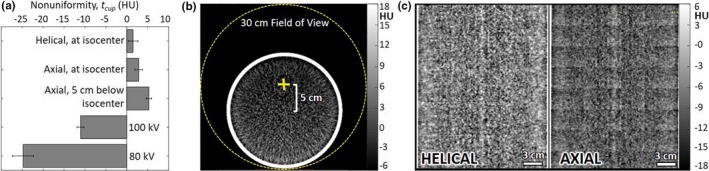
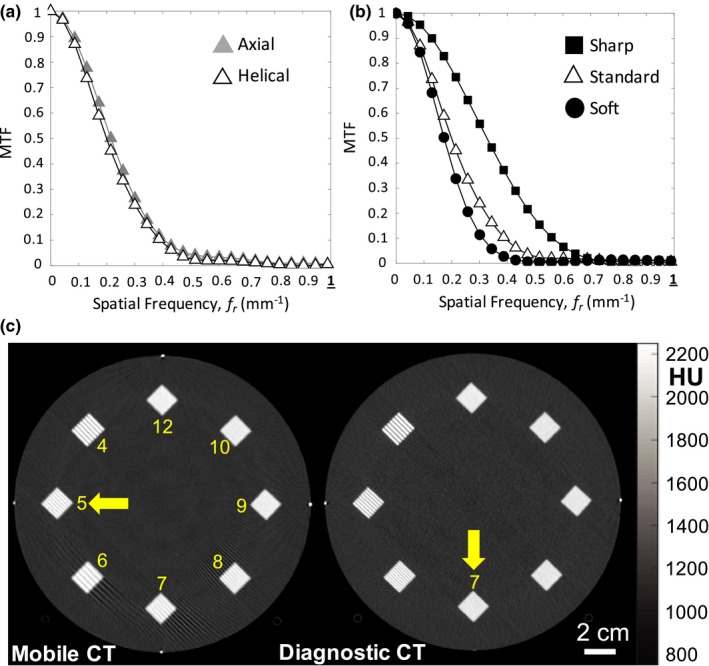
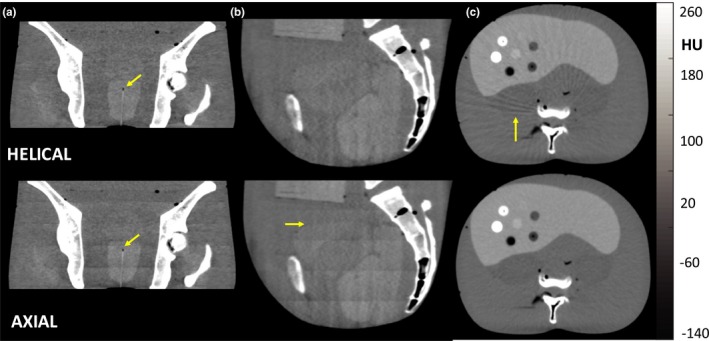
Result: Nominal dose for helical and axial modes, respectively, was 56.4 and 78.9 mGy for the head protocol and 17.8 and 24.9 mGy for the body protocol. A high degree of HU accuracy and linearity was observed for both axial and helical scan modes. Image nonuniformity (e.g., cupping artifact) in the transverse (x,y) plane was less than 5 HU, but stitching artifacts (~5 HU) in the longitudinal (z) direction were observed in axial scan mode. Helical and axial modes demonstrated comparable spatial resolution of ~5 lp/cm, with the MTF reduced to 10% at ~0.38 mm-1 . Contrast-to-noise ratio was suitable to soft-tissue visualization (e.g., fat and muscle), but windmill artifacts were observed in helical mode in relation to high-frequency bone and metal. The MAR algorithm provided modest improvement to image quality. Overall, image quality appeared suitable to relevant clinical tasks in intracavitary and interstitial (e.g., gynecological) brachytherapy, including visualization of soft-tissue structures in proximity to the applicators.
Conclusion: The technical assessment highlighted key characteristics of dose and imaging performance pertinent to incorporation of the mobile CT scanner in clinical procedures, helping to inform clinical deployment and technique protocol selection in brachytherapy. For this and other possible applications, the work helps to identify protocols that could reduce radiation dose and/or improve image quality. The work also identified areas for future improvement, including reduction of stitching, windmill, and metal artifacts.
Keywords: brachytherapy; dose; image guidance; image quality; mobile CT.
© 2019 The Authors. Journal of Applied Clinical Medical Physics published by Wiley Periodicals, Inc. on behalf of American Association of Physicists in Medicine.
Conflict of interest statement
No conflict of interest.
Figures
Similar articles
-
Technical assessment of a cone-beam CT scanner for otolaryngology imaging: image quality, dose, and technique protocols.Med Phys. 2012 Aug;39(8):4932-42. doi: 10.1118/1.4736805. Med Phys. 2012. PMID: 22894419
-
CT head-scan dosimetry in an anthropomorphic phantom and associated measurement of ACR accreditation-phantom imaging metrics under clinically representative scan conditions.Med Phys. 2013 Aug;40(8):081917. doi: 10.1118/1.4815964. Med Phys. 2013. PMID: 23927331
-
Characteristics and clinical application of a treatment simulator with Ct-option.Radiother Oncol. 1999 Mar;50(3):355-66. doi: 10.1016/s0167-8140(99)00033-x. Radiother Oncol. 1999. PMID: 10392823
-
Milestones in CT: Past, Present, and Future.Radiology. 2023 Oct;309(1):e230803. doi: 10.1148/radiol.230803. Radiology. 2023. PMID: 37847140 Free PMC article. Review.
-
Reducing the Energy Consumption of Magnetic Resonance Imaging and Computed Tomography Scanners: Integrating Ecodesign and Sustainable Operations.J Comput Assist Tomogr. 2025 Mar-Apr 01;49(2):191-202. doi: 10.1097/RCT.0000000000001700. Epub 2024 Dec 5. J Comput Assist Tomogr. 2025. PMID: 39631748 Review.
Cited by
-
Treatment of pediatric vaginal rhabdomyosarcoma with the use of a real-time tracked custom applicator.Brachytherapy. 2022 May-Jun;21(3):291-299. doi: 10.1016/j.brachy.2021.05.006. Epub 2022 Mar 18. Brachytherapy. 2022. PMID: 35623721 Free PMC article.
-
Assessment of needle bending and tracking requirements for optimized needle placement in combined intracavitary/interstitial gynecologic brachytherapy.Strahlenther Onkol. 2025 Feb 6. doi: 10.1007/s00066-025-02367-2. Online ahead of print. Strahlenther Onkol. 2025. PMID: 39915305
-
First clinical experience with a novel, mobile cone-beam CT system for treatment quality assurance in brachytherapy.Strahlenther Onkol. 2022 Jun;198(6):573-581. doi: 10.1007/s00066-022-01912-7. Epub 2022 Mar 12. Strahlenther Onkol. 2022. PMID: 35278094 Free PMC article.
-
Intraoperative radiation therapy with 50 kV x-rays: A multi-institutional review.J Appl Clin Med Phys. 2024 Mar;25(3):e14272. doi: 10.1002/acm2.14272. Epub 2024 Jan 26. J Appl Clin Med Phys. 2024. PMID: 38279520 Free PMC article. Review.
-
Open-source deep-learning models for segmentation of normal structures for prostatic and gynecological high-dose-rate brachytherapy: Comparison of architectures.J Appl Clin Med Phys. 2025 Jun;26(6):e70089. doi: 10.1002/acm2.70089. Epub 2025 Apr 5. J Appl Clin Med Phys. 2025. PMID: 40186596 Free PMC article.
References
-
- Weir VJ, Zhang J, Bruner AP. Dosimetric characterization and image quality evaluation of the AIRO mobile CT scanner. J X‐Ray Sci Technol. 2015;23:373–381. - PubMed
-
- Hecht N, Kamphuis M, Czabanka M, et al. Accuracy and workflow of navigated spinal instrumentation with the mobile AIRO (®) CT scanner. Eur Spine J. 2016;25:716–723. - PubMed
-
- Scarone P, Vincenzo G, Distefano D, et al. Use of the Airo mobile intraoperative CT system versus the O‐arm for transpedicular screw fixation in the thoracic and lumbar spine: a retrospective cohort study of 263 patients. J Neurosurg Spine. 2018;29:397–406. - PubMed
-
- Viswanathan AN, Thomadsen B, and American Brachytherapy Society Cervical Cancer Recommendations Committee . American Brachytherapy consensus guidelines for locally advanced carcinoma of the cervix. Part I: general principles. Brachytherapy. 2012;11:33–46. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
