

The mechanisms of acute interstitial nephritis in the era of immune checkpoint inhibitors in melanoma
- PMID: 31579108
- PMCID: PMC6759704
- DOI: 10.1177/1758835919875549
The mechanisms of acute interstitial nephritis in the era of immune checkpoint inhibitors in melanoma
Erratum in
-
CORRIGENDUM to The mechanisms of acute interstitial nephritis in the era of immune checkpoint inhibitors in melanoma.Ther Adv Med Oncol. 2019 Oct 18;11:1758835919885202. doi: 10.1177/1758835919885202. eCollection 2019. Ther Adv Med Oncol. 2019. PMID: 31666813 Free PMC article.
Abstract
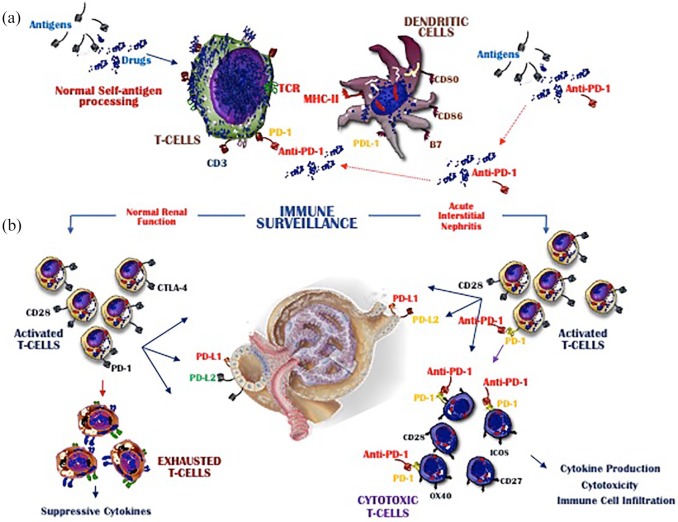
Treatment with immune checkpoint inhibitors (ICIs) has improved the prognosis of patients with a number of types of cancer, but the frequent development of immune-related adverse effects (irAEs) can worsen the outcome. The most common irAEs involve the gastrointestinal, cutaneous, and endocrine systems, but nephrotoxicity, resulting from damage to the tubule-interstitial compartment, may occur in some patients. The early phases of acute interstitial nephritis (AIN) are characterized by systemic symptoms that indicate a poor clinical state as well as a mild deterioration of renal function. Tubular injury is due to a direct effect mediated by cytotoxic CD8+ T cells, which sustain the local production of pro-inflammatory cytokines that progressively impair renal function. The treatment of AIN is mainly based on high-dose steroids, which in most instances leads to the recovery of renal function. However, the premature discontinuation of ICI therapy may prevent the impact of treatment on the clinical progression of the malignancy. Adequately addressing irAEs requires a standardized therapy that is based on the results of large clinical trials.
Keywords: acute interstitial nephritis; immunotherapy; melanoma; nephrotoxicity.
© The Author(s), 2019.
Conflict of interest statement
Conflict of interest statement: The authors declare that there is no conflict of interest.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer Statistics, 2017. CA Cancer J Clin 2017; 67: 7–30. - PubMed
-
- Arenas-Ramirez N, Woytschak J, Boyman O. Interleukin-2: biology, design and application. Trends Immunol 2015; 36: 763–777. - PubMed
-
- Robert C, Long GV, Brady B, et al. Nivolumab in previously untreated melanoma without BRAF mutation. N Engl J Med 2015; 372: 320–330. - PubMed
-
- Robert C, Ribas A, Wolchok JD, et al. Anti-programmed-death-receptor-1 treatment with pembrolizumab in ipilimumab-refractory advanced melanoma: a randomised dose-comparison cohort of a phase 1 trial. Lancet 2014; 384: 1109–1117. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
