

Survival trends of grade I, II, and III astrocytoma patients and associated clinical practice patterns between 1999 and 2010: A SEER-based analysis
- PMID: 31579519
- PMCID: PMC6760339
- DOI: 10.1093/nop/npv016
Survival trends of grade I, II, and III astrocytoma patients and associated clinical practice patterns between 1999 and 2010: A SEER-based analysis
Abstract
Background: The survival trends and the patterns of clinical practice pertaining to radiation therapy and surgical resection for WHO grade I, II, and III astrocytoma patients remain poorly characterized.
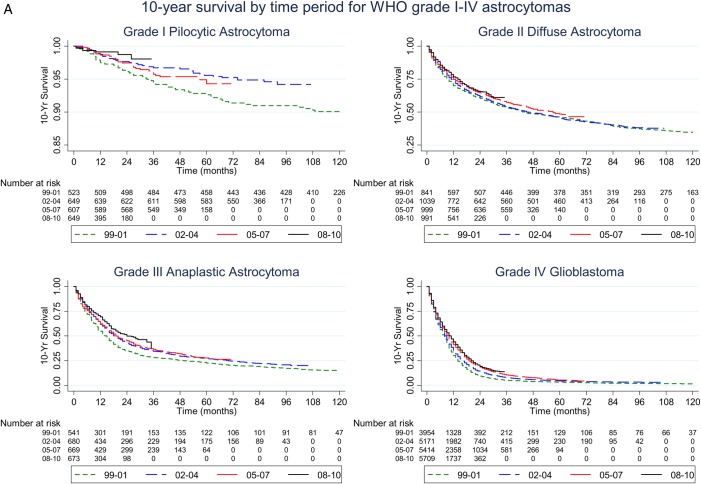
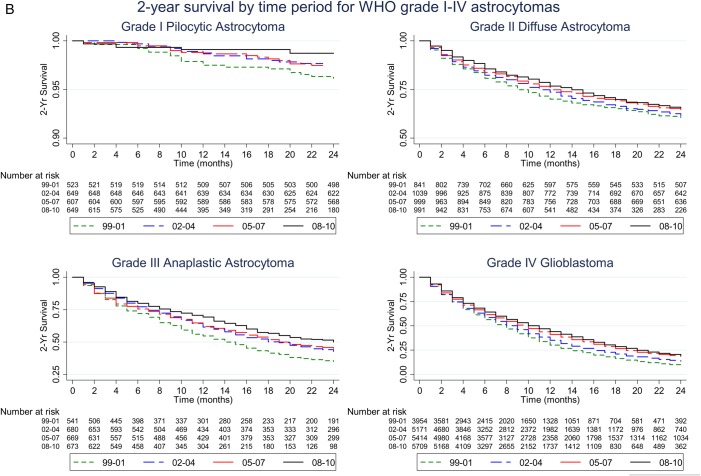
Methods: Using the Surveillance, Epidemiology and End Results (SEER) database, we identified 2497 grade I, 4113 grade II, and 2755 grade III astrocytomas during the period of 1999-2010. Time-trend analyses were performed for overall survival, radiation treatment (RT), and the extent of surgical resection (EOR).
Results: While overall survival of grade I astrocytoma patients remained unchanged during the study period, we observed improved overall survival for grade II and III astrocytoma patients (Tarone-Ware P < .05). The median survival increased from 44 to 57 months and from 15 to 24 months for grade II and III astrocytoma patients, respectively. The differences in survival remained significant after adjusting for pertinent variables including age, ethnicity, marital status, sex, tumor size, tumor location, EOR, and RT status. The pattern of clinical practice in terms of EOR for grade II and III astrocytoma patients did not change significantly during this study period. However, there was decreased RT utilization as treatment for grade II astrocytoma patients after 2005.
Conclusion: Results from the SEER database indicate that there were improvements in the overall survival of grade II and III astrocytoma patients over the past decade. Analysis of the clinical practice patterns identified potential opportunities for impacting the clinical course of these patients.
Keywords: WHO grade I, II, III astrocytomas; population-based SEER database; practice pattern; survival.
© The Author(s) 2015. Published by Oxford University Press on behalf of the Society for Neuro-Oncology. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Bartek J Jr., Ng K, Bartek J et al. Key concepts in glioblastoma therapy. J Neurol Neurosurg Psychiatry. 2012;83(7):753–760. - PubMed
-
- Ng K, Kim R, Kesari S et al. Genomic profiling of glioblastoma: convergence of fundamental biologic tenets and novel insights. J Neurooncol. 2012;107(1):1–12. - PubMed
-
- Ohgaki H, Kleihues P. Epidemiology and etiology of gliomas. Acta Neuropathol. 2005;109(1):93–108. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
