

Direct Superior Approach to the Hip for Total Hip Arthroplasty
- PMID: 31579535
- PMCID: PMC6687490
- DOI: 10.2106/JBJS.ST.18.00078
Direct Superior Approach to the Hip for Total Hip Arthroplasty
Abstract
Background: Traditional posterior approaches to the hip, posterolateral and mini-posterior, violate the iliotibial band and the short external rotators, specifically the quadratus femoris and obturator externus muscles1-4. The direct anterior approach does not violate the iliotibial band or the quadratus femoris, resulting in earlier ambulation and lower dislocation rates1,5-9. The direct superior (DS) is a posterior approach that spares the iliotibial band, obturator externus tendon, and quadratus femoris muscle. The goal of minimally invasive surgery (MIS) is to disrupt the least amount of tissue necessary to adequately expose the hip and correctly place implants. Although MIS total hip arthroplasty (THA) has not lived up to all of its promises10-13, MIS-THA may enable early ambulation and decrease length of stay14-16.
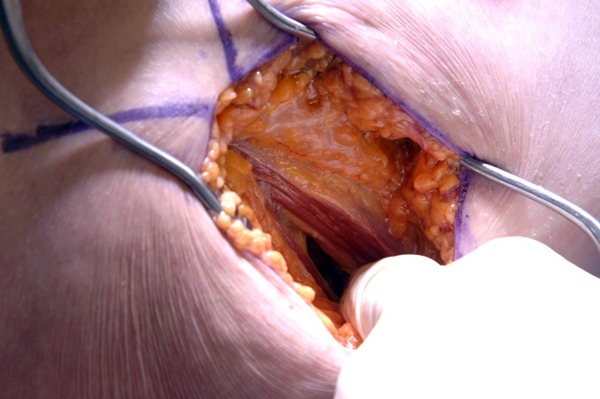
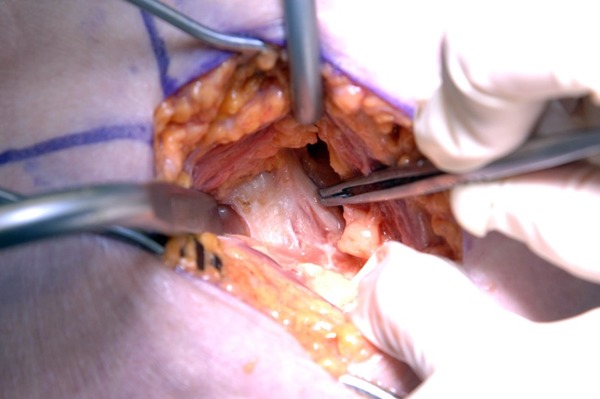
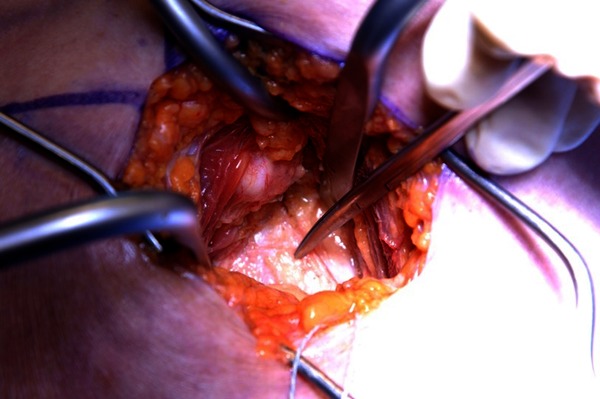
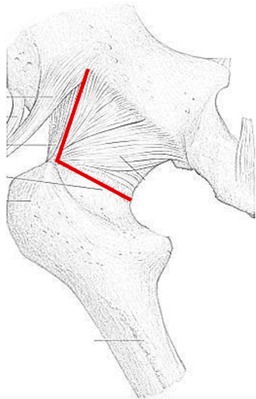
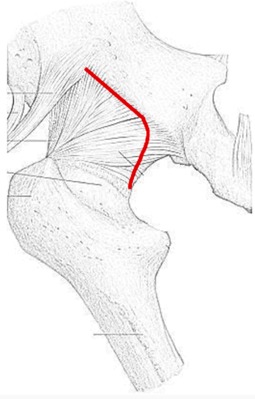
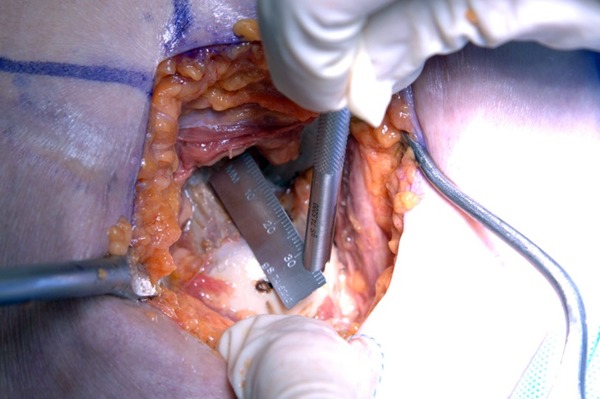
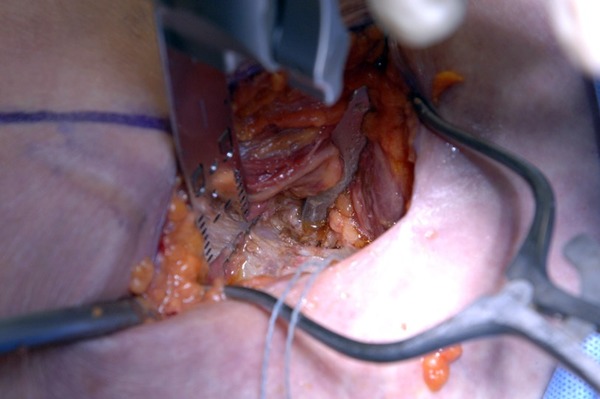
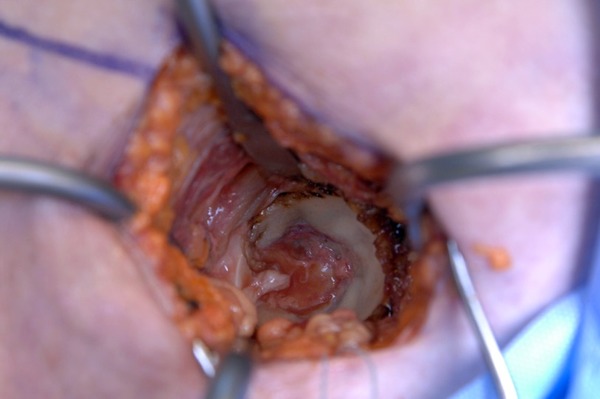
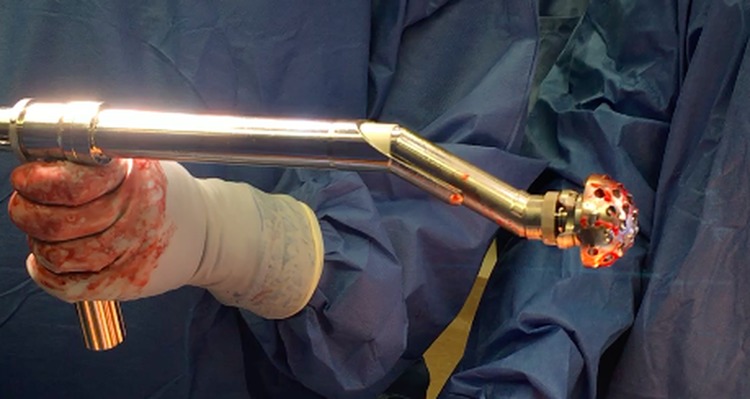
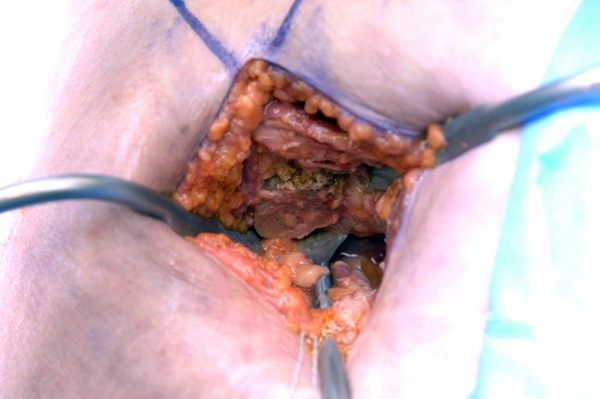
Description: The patient is positioned in the lateral decubitus position. An 8 to 10-cm incision is made at a 60° oblique angle starting from the posterior-proximal corner of the greater trochanter. Only the gluteus maximus fascia is incised; the Iliotibial band is completely spared. The gluteus maximus muscle is split bluntly, exposing the gluteus medius muscle, piriformis tendon, and triceps coxae (the obturator internus and superior and inferior gemellus muscles). The piriformis and conjoined tendon are released from the greater trochanter and tagged. The gluteus minimus is elevated, exposing the posterior hip capsule. An arthrotomy is performed prior to dislocating the hip with flexion, adduction, internal rotation, and axial compression. The femoral neck is resected, the acetabulum is reamed, and components or trials are impacted into position. Hip stability is assessed. Final implants are placed. The posterior capsule, piriformis, and obturator internus tendons are repaired anatomically. The fascia and skin are closed.
Alternatives: Posterolateral approach.Mini-posterior approach.Direct lateral approach.Anterolateral approach.Percutaneously assisted total hip (PATH).Supercapsular PATH (SuperPath).
Rationale: The DS approach to the hip differs from the traditional posterior and mini-posterior approaches because it preserves the iliotibial band, quadratus femoris muscle, and obturator externus tendon1, potentially suppressing dislocation. The DS approach to the hip causes less soft-tissue destruction, especially to the gluteus minimus and tensor fasciae latae muscles, compared with the direct anterior approach to the hip, suggesting DS-THA may enhance postoperative mobility1,3,14-16. DS-THA is extensile by extending the incision distally, incising the iliotibial band, and releasing the quadratus femoris muscle. This converts a DS approach to a standard posterolateral approach, providing additional visualization.
Copyright © 2019 by The Journal of Bone and Joint Surgery, Incorporated.
Figures






References
-
- Amanatullah DF, Masini MA, Roger DJ, Pagnano MW. Greater inadvertent muscle damage in direct anterior approach when compared with the direct superior approach for total hip arthroplasty. Bone Joint J. 2016. August;98-B(8):1036-42. - PubMed
-
- Mardones R, Pagnano MW, Nemanich JP, Trousdale RT. The Frank Stinchfield Award: muscle damage after total hip arthroplasty done with the two-incision and mini-posterior techniques. Clin Orthop Relat Res. 2005. December;441:63-7. - PubMed
-
- Solomon LB, Lee YC, Callary SA, Beck M, Howie DW. Anatomy of piriformis, obturator internus and obturator externus: implications for the posterior surgical approach to the hip. J Bone Joint Surg Br. 2010. September;92(9):1317-24. - PubMed
-
- Martin CT, Pugely AJ, Gao Y, Clark CR. A comparison of hospital length of stay and short-term morbidity between the anterior and the posterior approaches to total hip arthroplasty. J Arthroplasty. 2013. May;28(5):849-54. Epub 2013 Mar 11. - PubMed
LinkOut - more resources
Full Text Sources