

Improving Quality of Chest Computed Tomography for Evaluation of Pediatric Malignancies
- PMID: 31579866
- PMCID: PMC6594776
- DOI: 10.1097/pq9.0000000000000166
Improving Quality of Chest Computed Tomography for Evaluation of Pediatric Malignancies
Abstract
Introduction: Atelectasis is a problem in sedated pediatric patients undergoing cross-sectional imaging, impairing the ability to accurately interpret chest computed tomography (CT) imaging for the presence of malignancy, often leading to additional maneuvers and/or repeat imaging with additional radiation exposure.
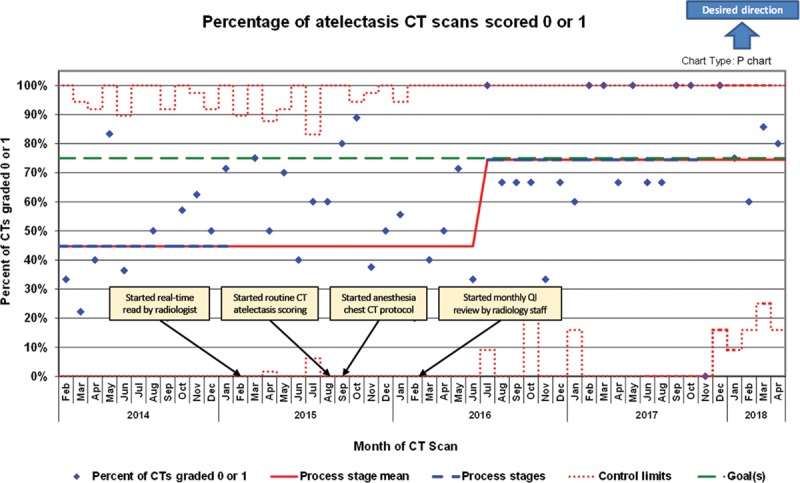
Methods: A quality improvement team established a best-practice protocol to improve the quality of thoracic CT imaging in young patients with suspected primary or metastatic pulmonary malignancy. The specific aim was to increase the percentage of chest CT scans obtained for the evaluation of pulmonary nodules with acceptable atelectasis scores (0-1) in patients aged 0-5 years with malignancy, from a baseline of 45% to a goal of 75%.
Results: A retrospective cohort consisted of 94 patients undergoing chest CT between February 2014 and January 2015 before protocol implementation. The prospective cohort included 195 patients imaged between February 2015 and April 2018. The baseline percentage of CT scans that were scored 0 or 1 on the atelectasis scale was 44.7%, which improved to 75% with protocol implementation. The mean atelectasis score improved from 1.79 (±0.14) to 0.7 (±0.09). Sedation incidence decreased substantially from 73.2% to 26.5% during the study period.
Conclusions: Using quality improvement methodology including standardization of care, the percentage of children with atelectasis scores of 0-1 undergoing cross-sectional thoracic imaging improved from 45% to 75%. Also, eliminating the need for sedation in these patients has further improved image quality, potentially allowing for optimal detection of smaller nodules, and minimizing morbidity.
Copyright © 2019 the Author(s). Published by Wolters Kluwer Health, Inc.
Figures





Similar articles
-
Ultrafast pediatric chest computed tomography: comparison of free-breathing vs. breath-hold imaging with and without anesthesia in young children.Pediatr Radiol. 2019 Mar;49(3):301-307. doi: 10.1007/s00247-018-4295-5. Epub 2018 Nov 9. Pediatr Radiol. 2019. PMID: 30413857
-
Chest CT in children: anesthesia and atelectasis.Pediatr Radiol. 2014 Feb;44(2):164-72. doi: 10.1007/s00247-013-2800-4. Epub 2013 Nov 8. Pediatr Radiol. 2014. PMID: 24202432 Clinical Trial.
-
Impact of airway and a standardized recruitment maneuver on CT chest imaging quality in a pediatric population: A retrospective review.Paediatr Anaesth. 2022 Apr;32(4):572-576. doi: 10.1111/pan.14341. Epub 2021 Nov 29. Paediatr Anaesth. 2022. PMID: 34811851
-
Thoracic imaging tests for the diagnosis of COVID-19.Cochrane Database Syst Rev. 2020 Nov 26;11:CD013639. doi: 10.1002/14651858.CD013639.pub3. Cochrane Database Syst Rev. 2020. Update in: Cochrane Database Syst Rev. 2021 Mar 16;3:CD013639. doi: 10.1002/14651858.CD013639.pub4. PMID: 33242342 Updated.
-
LUCIS: lung cancer imaging studies.Dan Med J. 2012 Nov;59(11):B4542. Dan Med J. 2012. PMID: 23171752 Review.
Cited by
-
Optimizing perioperative lung protection strategies for reducing postoperative respiratory complications in pediatric patients: a narrative review.Transl Pediatr. 2024 Nov 30;13(11):2043-2058. doi: 10.21037/tp-24-453. Epub 2024 Nov 26. Transl Pediatr. 2024. PMID: 39649647 Free PMC article. Review.
References
-
- Damgaard-Pedersen K, Qvist T. Pediatric pulmonary CT-scanning. Anaesthesia-induced changes. Pediatr Radiol. 1980;9:145–148. - PubMed
-
- Newman B, Krane EJ, Gawande R, et al. Chest CT in children: anesthesia and atelectasis. Pediatr Radiol. 2014;44:164–172. - PubMed
-
- Sargent MA, McEachern AM, Jamieson DH, et al. Atelectasis on pediatric chest CT: comparison of sedation techniques. Pediatr Radiol. 1999;29:509–513. - PubMed
-
- Lam WW, Chen PP, So NM, et al. Sedation versus general anaesthesia in paediatric patients undergoing chest CT. Acta Radiol. 1998;39:298–300. - PubMed
-
- Sargent MA, Jamieson DH, McEachern AM, et al. Increased inspiratory pressure for reduction of atelectasis in children anesthetized for CT scan. Pediatr Radiol. 2002;32:344–347. - PubMed
LinkOut - more resources
Full Text Sources
Miscellaneous