

Early mobilization of critically ill patients in the intensive care unit: A systematic review and meta-analysis
- PMID: 31581205
- PMCID: PMC6776357
- DOI: 10.1371/journal.pone.0223185
Early mobilization of critically ill patients in the intensive care unit: A systematic review and meta-analysis
Abstract
Background: Physical therapy can prevent functional impairments and improve the quality of life of patients after hospital discharge. However, the effect of early mobilization on patients with a critical illness remains unclear. This study was performed to assess the evidence available regarding the effect of early mobilization on critically ill patients in the intensive care unit (ICU).
Methods: Electronic databases were searched from their inception to March 21, 2019. Randomized controlled trials (RCTs) comprising critically ill patients who received early mobilization were included. The methodological quality and risk of bias of each eligible trial were assessed using the Cochrane Collaboration tool. Data were extracted using a standard collection form each included study, and processed using the Mantel-Haenszel (M-H) or inverse-variance (I-V) test in the STATA v12.0 statistical software.
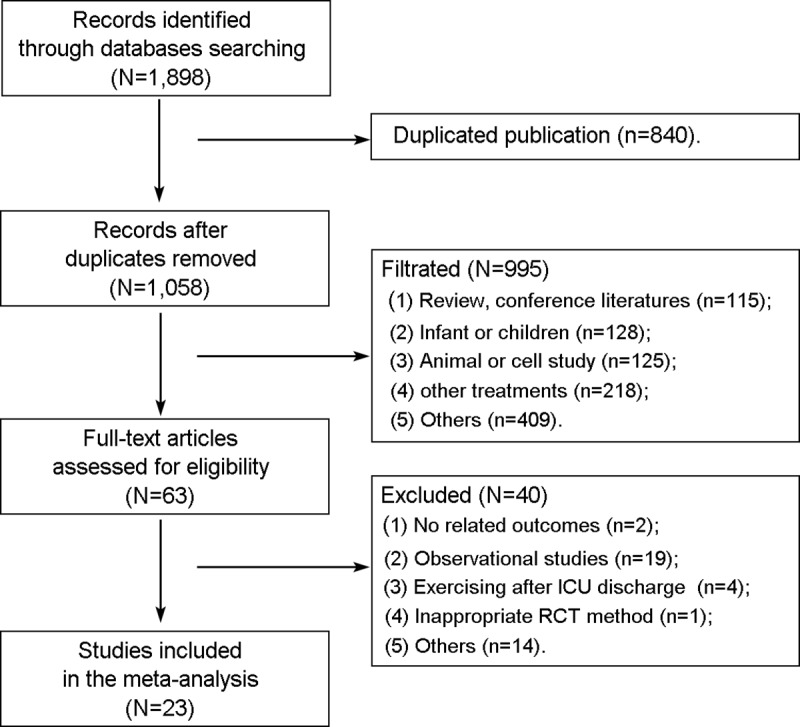
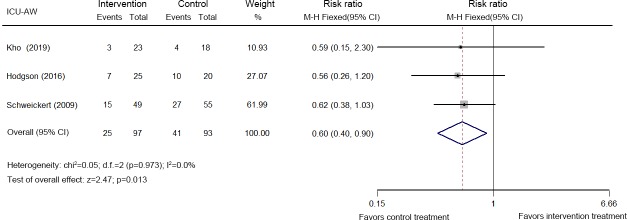
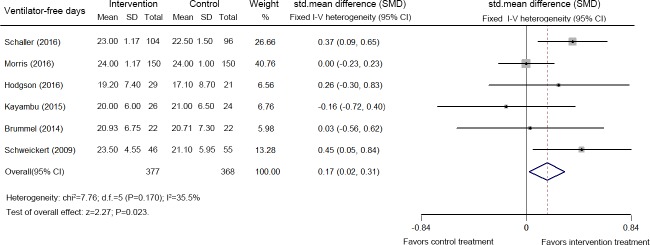
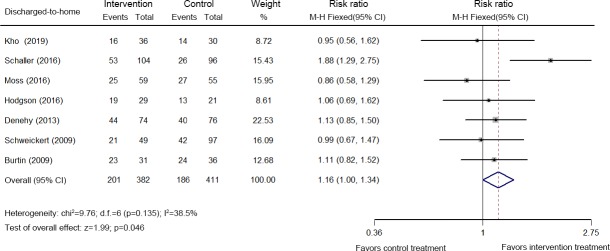
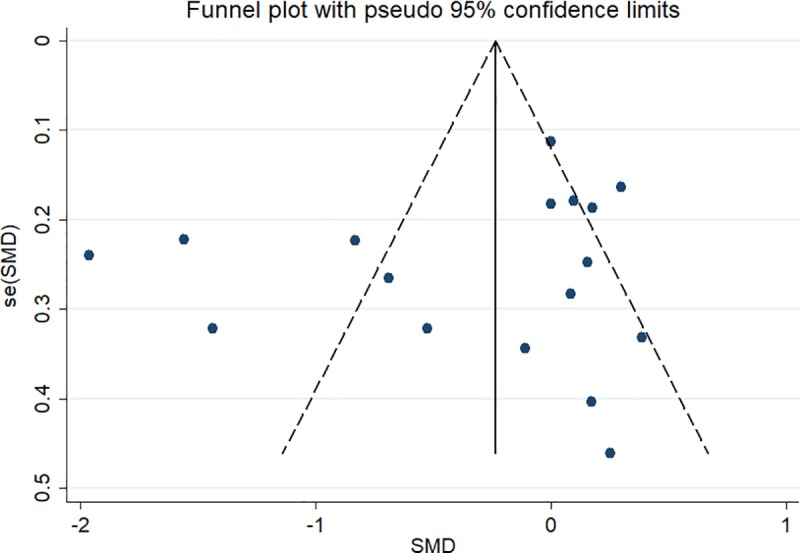
Results: A total of 1,898 records were screened. Twenty-three RCTs comprising 2,308 critically ill patients were ultimately included. Early mobilization decreased the incidence of ICU-acquired weakness (ICU-AW) at hospital discharge (three studies, 190 patients, relative risk (RR): 0.60, 95% confidence interval (CI) [0.40, 0.90]; p = 0.013, I2 = 0.0%), increased the number of patients who were able to stand (one study, 50 patients, 90% vs. 62%, p = 0.02), increased the number of ventilator-free days (six studies, 745 patients, standardized mean difference (SMD): 0.17, 95% CI [0.02, 0.31]; p = 0.023, I2 = 35.5%) during hospitalization, increased the distance the patient was able to walk unassisted (one study, 104 patients, 33.4 (0-91.4) meters vs. 0 (0-30.4) meters, p = 0.004) at hospital discharge, and increased the discharged-to-home rate (seven studies, 793 patients, RR: 1.16, 95% CI [1.00, 1.34]; p = 0.046). The mortality (28-day, ICU and hospital) and adverse event rates were moderately increased by early mobilization, but the differences were statistically non-significant. However, due to the substantial heterogeneity among the included studies, and the low quality of the evidence, the results of this study should be interpreted with caution. Publication bias was not identified.
Conclusions: Early mobilization appears to decrease the incidence of ICU-AW, improve the functional capacity, and increase the number of ventilator-free days and the discharged-to-home rate for patients with a critical illness in the ICU setting.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
