

Glycemic Index, Glycemic Load and Cancer Risk: An Updated Meta-Analysis
- PMID: 31581675
- PMCID: PMC6835610
- DOI: 10.3390/nu11102342
Glycemic Index, Glycemic Load and Cancer Risk: An Updated Meta-Analysis
Abstract
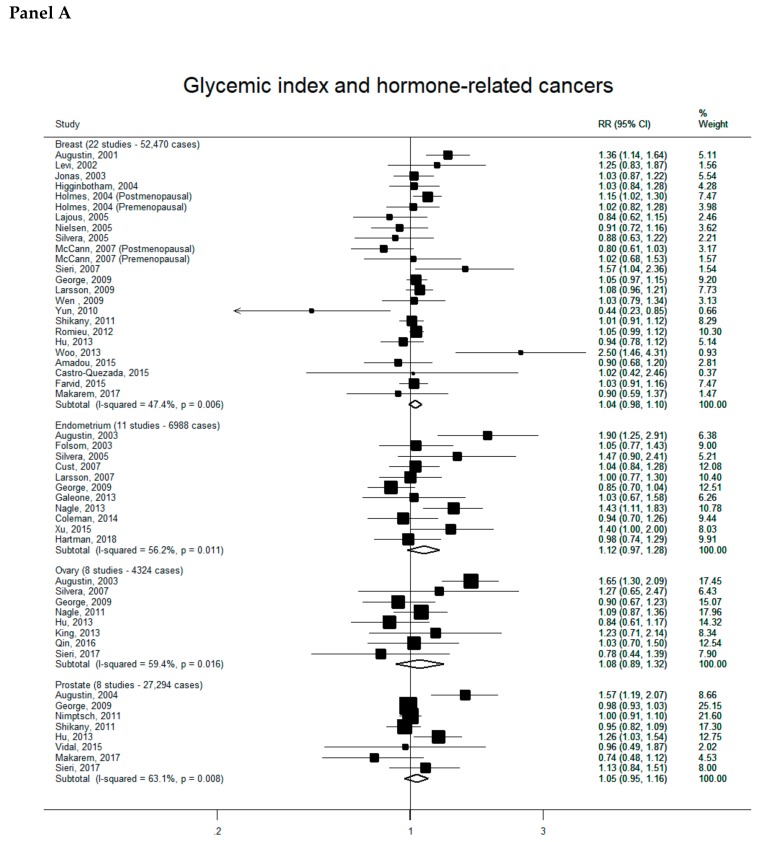
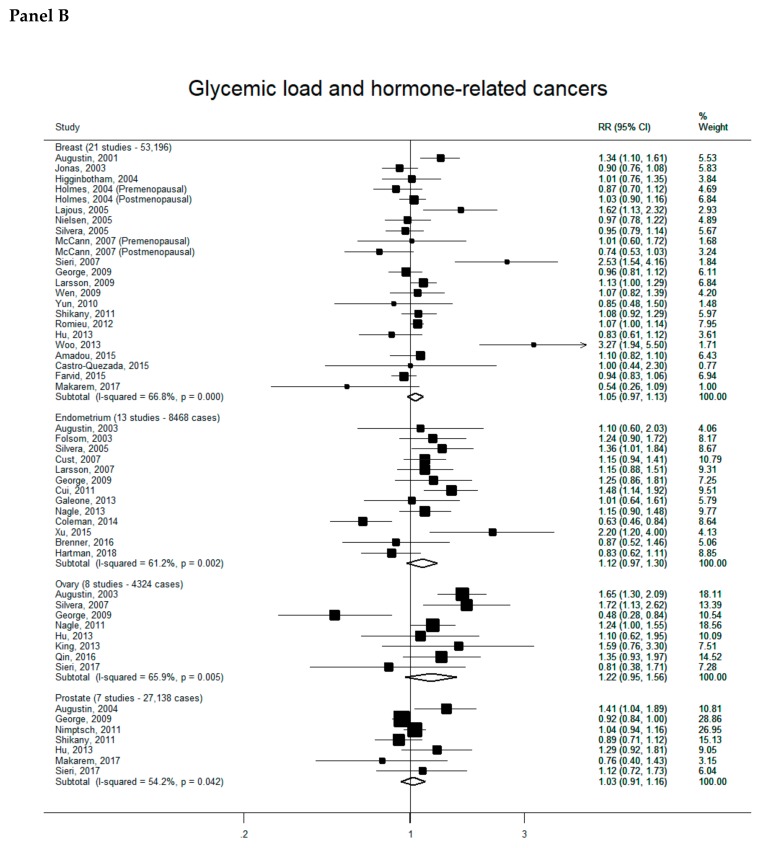
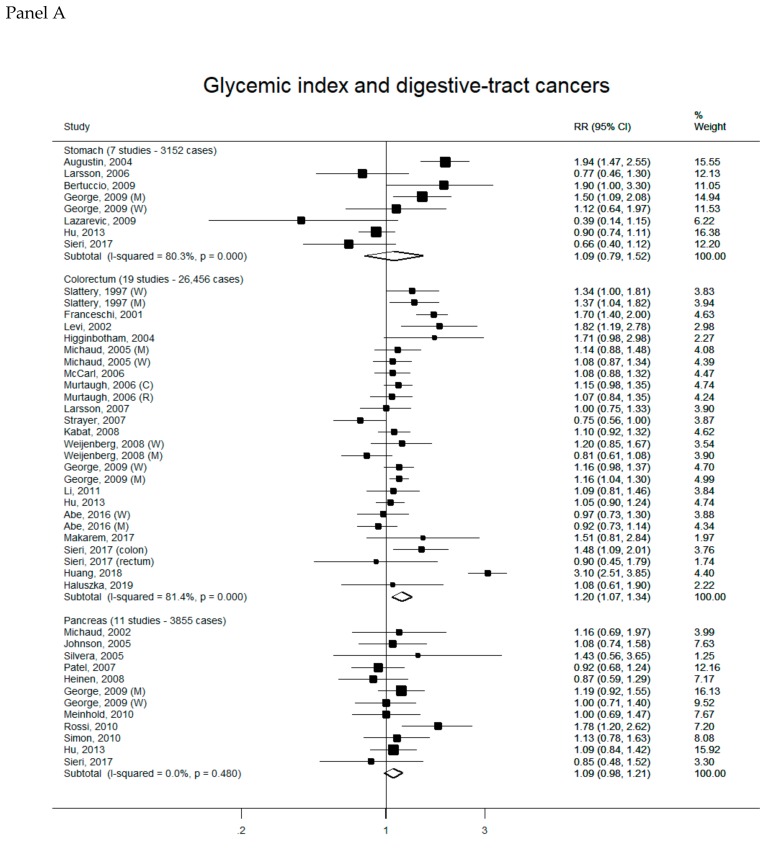
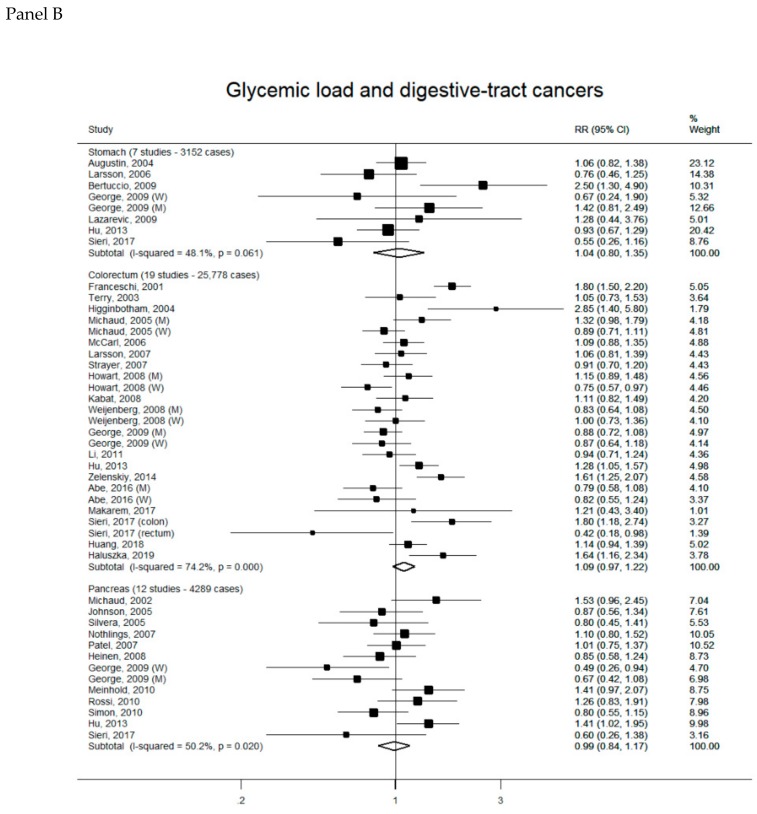
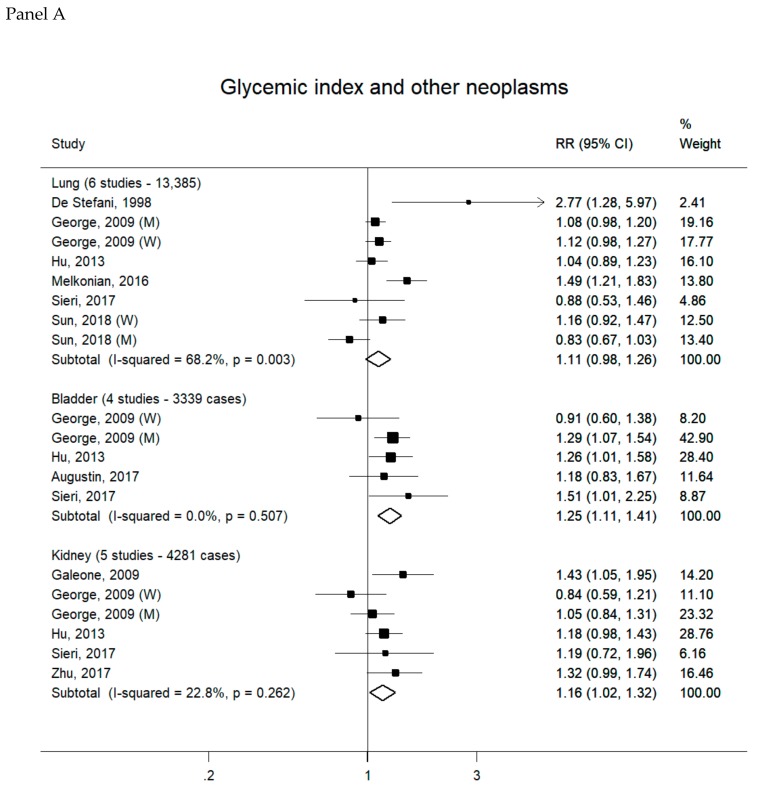
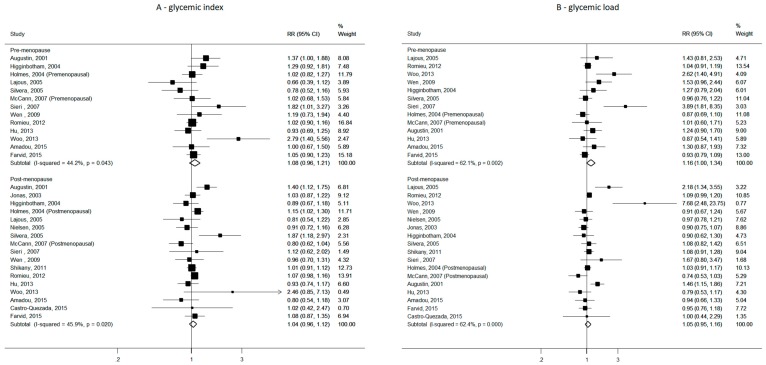
Diets high in glycemic index (GI) and glycemic load (GL) have been related to an increased risk of selected cancers, but additional quantification is required. We updated a systematic review and meta-analysis published in 2015 to May 2019 to provide quantitative information on GI/GL and cancer risk. Relative risks (RR) and the corresponding 95 % confidence intervals (CI) for the highest versus the lowest categories of GI and GL were extracted from selected studies and pooled using random-effects models. Twenty reports (>22,000 cancer cases) have become available after January 2015, and 15 were added to the meta-analyses by cancer sites, which considered a total of 88 investigations. The five additional reports were reviewed, but not included in the meta-analyses, since data were inadequate to be pooled. For hormone-related cancers, summary RRs for the highest versus lowest GI and GL intakes were moderately increased. They ranged from 1.04 (breast) to 1.12 (endometrium) for GI and from 1.03 (prostate) to 1.22 (ovary) for GL, of borderline significance. High GI was associated with small increased risks of colorectal (summary RR for GI: 1.20, 95% CI, 1.07-1.34-GL: 1.09, 95% CI, 0.97-1.22, 19 studies), bladder (GI: 1.25, 95% CI, 1.11-1.41-GL: 1.10, 95% CI, 0.85-1.42, four studies) and kidney cancers (GI: 1.16, 95% CI, 1.02-1.32-GL: 1.14, 95% CI, 0.81-1.60, five studies). GL was not significantly related to those cancer sites. Stomach, prostate and lung cancers were not associated with GI and GL. The present analysis, based on an updated comprehensive evaluation of the epidemiological literature, indicates moderate unfavorable effects of high versus low GI on colorectal, and possibly bladder and kidney cancers, and a possible moderate positive association between GL and endometrial cancer.
Keywords: cancer; glycemic index; glycemic load; review; risk.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Augustin L.S., Kendall C.W., Jenkins D.J., Willett W.C., Astrup A., Barclay A.W., Bjorck I., Brand-Miller J.C., Brighenti F., Buyken A.E., et al. Glycemic index, glycemic load and glycemic response: An international scientific consensus summit from the international carbohydrate quality consortium (icqc) Nutr. Metab. Cardiovasc. Dis. 2015;25:795–815. doi: 10.1016/j.numecd.2015.05.005. - DOI - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
