

Lung Ultrasound in Acute Heart Failure: Prevalence of Pulmonary Congestion and Short- and Long-Term Outcomes
- PMID: 31582107
- PMCID: PMC8409324
- DOI: 10.1016/j.jchf.2019.07.008
Lung Ultrasound in Acute Heart Failure: Prevalence of Pulmonary Congestion and Short- and Long-Term Outcomes
Abstract
Objectives: This study sought to assess the prevalence, changes in, and prognostic importance of B-lines, a pulmonary congestion measure by using a simplified lung ultrasonography (LUS) method in acute heart failure (AHF).
Background: Pulmonary congestion is an important finding in AHF, but conventional methods for its detection are insensitive.
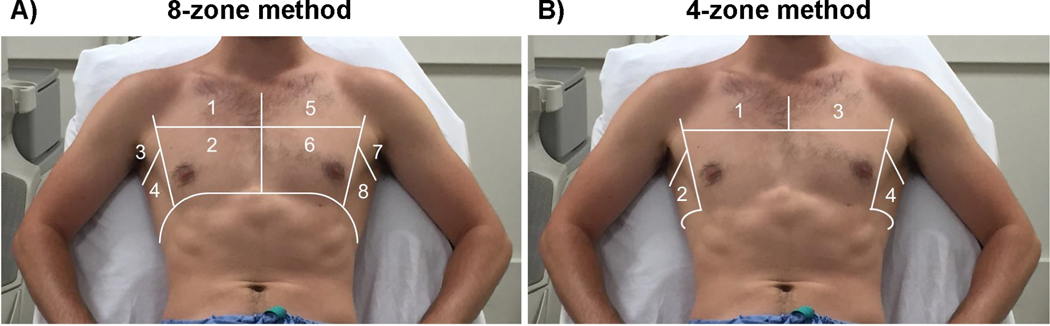
Methods: In a 2-site, prospective, observational study, 4-zone LUS was performed early during hospitalization for AHF (LUS1) and at discharge (LUS2). B-lines were quantified off-line, blinded to clinical findings and outcomes, by a core laboratory.
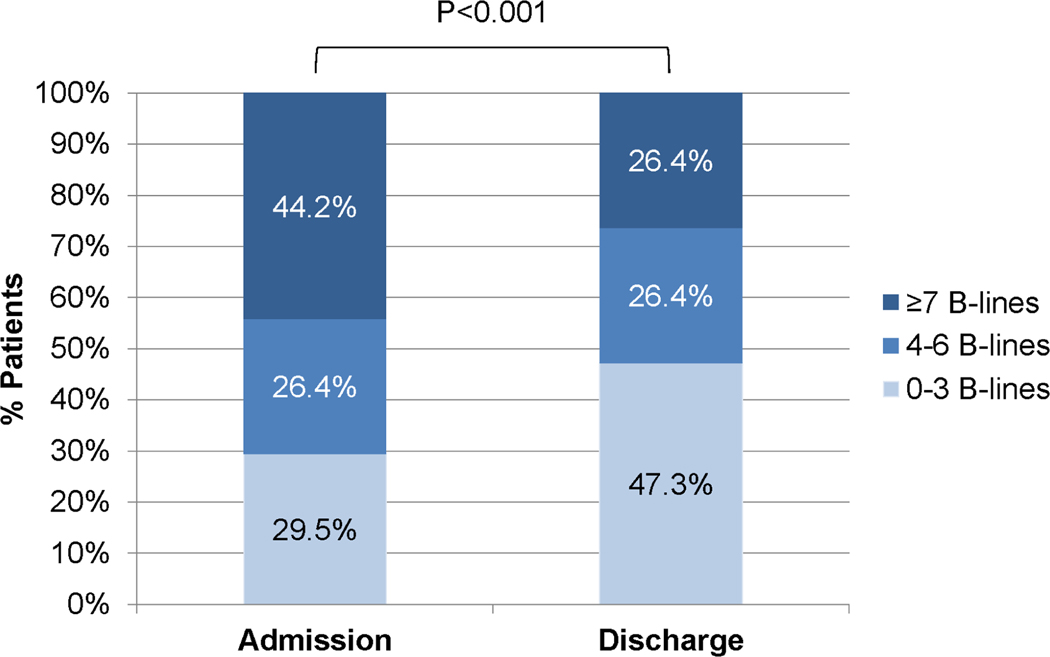
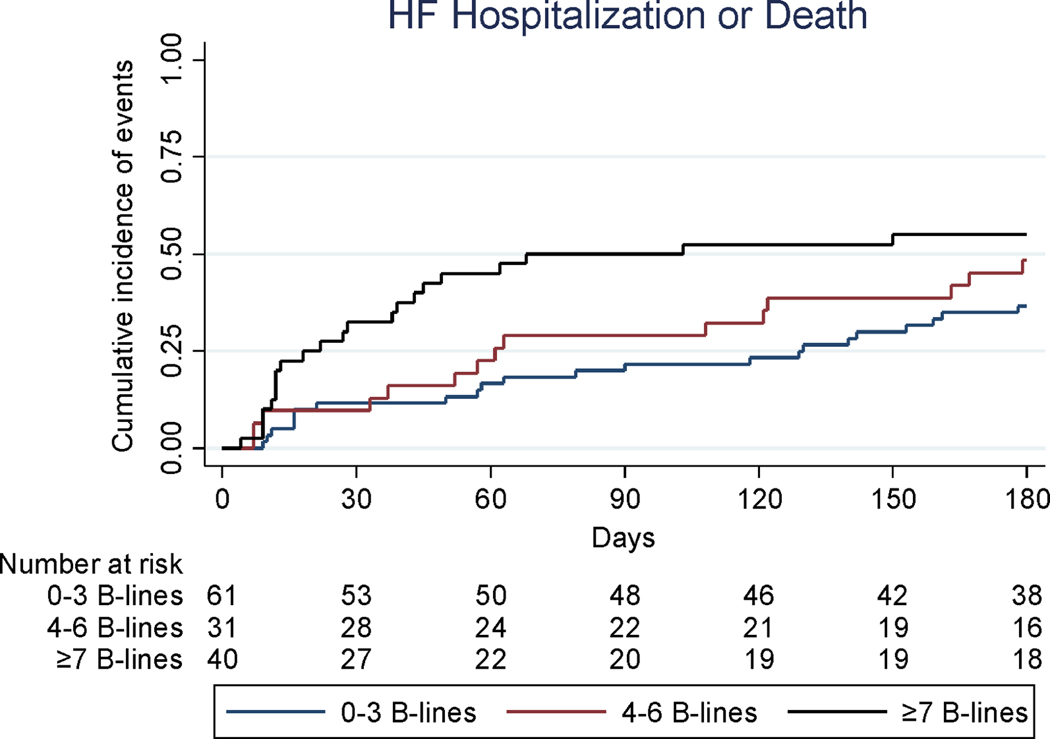
Results: Among 349 patients (median, 75 years of age; 59% men; mean ejection fraction 39%), the sum of B-lines in 4 zones ranged from 0 to 18 (LUS1). The risk of an adverse in-hospital event increased with rising number of B-lines on LUS1: the odds ratio for each B-line tertile was 1.82 (95% confidence interval [CI]: 1.14 to 2.88; p = 0.011). B-line count decreased from a median of 6 (LUS1) to 4 (LUS2; p < 0.001) over 6 days (median). In 132 patients with LUS2 images, the risk of HF hospitalization or all-cause death was greater in patients with a higher number of B-lines at discharge. This relationship was stronger closer to discharge: unadjusted hazard ratio (HR) at 60 days was 3.30 (95% CI: 1.52 to 7.17; p = 0.002); 2.94 at 90 days (95% CI: 1.46 to 5.93; p = 0.003); and 2.01 at 180 days (95% CI: 1.11 to 3.64; p = 0.021). The association between number of B-lines and short- and long-term outcomes persisted after adjusting for important clinical variables, including N-terminal pro-B-type natriuretic peptide.
Conclusions: Pulmonary congestion using a simplified 4-zone LUS method was common in patients with AHF and improved with therapy. A higher number of B-lines at baseline and discharge identified patients at increased risk for adverse events.
Keywords: acute heart failure; lung ultrasonography; prognosis; pulmonary congestion.
Copyright © 2019 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
Conflict of Interest:
all other authors report no relevant conflicts of interest.
Figures
Comment in
-
Lung Ultrasound: Our New "Sixth Sense"?JACC Heart Fail. 2019 Oct;7(10):859-861. doi: 10.1016/j.jchf.2019.08.006. JACC Heart Fail. 2019. PMID: 31582108 No abstract available.
References
-
- Wang CS, FitzGerald JM, Schulzer M, et al.Does this dyspneic patient in the emergency department have congestive heart failure? JAMA. 2005;294:1944–56. - PubMed
-
- Ambrosy AP, Pang PS, Khan S, et al.Clinical course and predictive value of congestion during hospitalization in patients admitted for worsening signs and symptoms of heart failure with reduced ejection fraction: findings from the EVEREST trial. Eur Heart J. 2013;34:835–43. - PubMed
-
- Butler J, Gheorghiade M, Metra M. Moving away from symptoms-based heart failure treatment: misperceptions and real risks for patients with heart failure. Eur J Heart Fail. 2016;18:350–2. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
