

Myeloablative vs reduced intensity T-cell-replete haploidentical transplantation for hematologic malignancy
- PMID: 31582392
- PMCID: PMC6784523
- DOI: 10.1182/bloodadvances.2019000627
Myeloablative vs reduced intensity T-cell-replete haploidentical transplantation for hematologic malignancy
Abstract
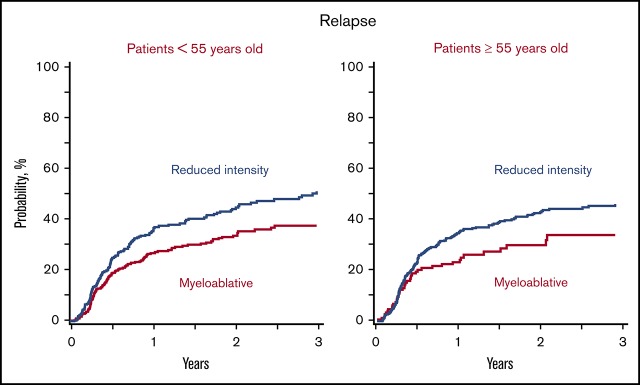
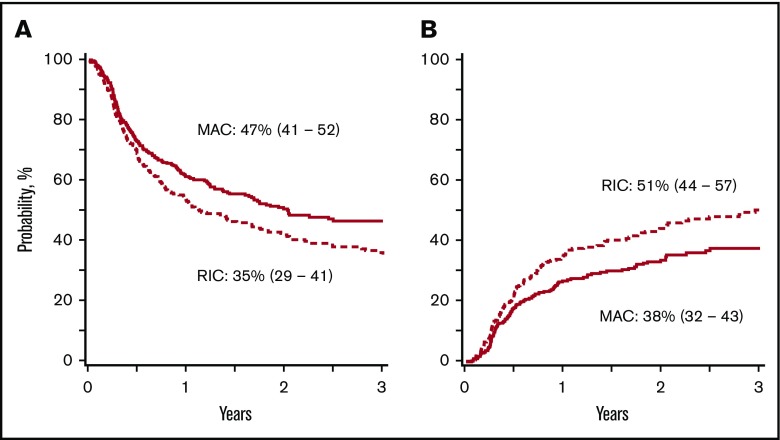
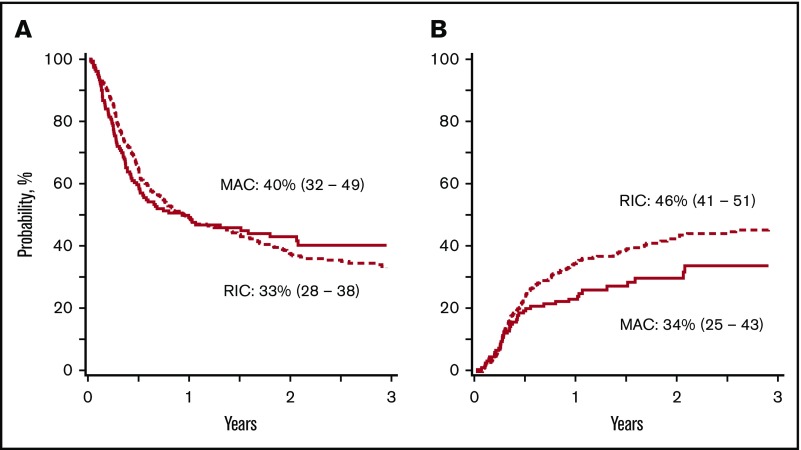
In the absence of prospective studies that examine the effect of conditioning regimen intensity after T-cell-replete haploidentical transplant for acute myeloid leukemia (AML), acute lymphoblastic leukemia (ALL), and myelodysplastic syndrome (MDS), a retrospective cohort analysis was performed. Of the 1325 eligible patients (AML, n = 818; ALL, n = 286; and MDS, n = 221), 526 patients received a myeloablative regimen and 799 received a reduced-intensity regimen. Graft-versus-host disease prophylaxis was uniform with posttransplant cyclophosphamide, a calcineurin inhibitor, and mycophenolate mofetil. The primary end point was disease-free survival. Cox regression models were built to study the effect of conditioning regimen intensity on transplant outcomes. For patients aged 18 to 54 years, disease-free survival was lower (hazard ratio [HR], 1.34; 42% vs 51%; P = .007) and relapse was higher (HR, 1.51; 44% vs 33%; P = .001) with a reduced-intensity regimen compared with a myeloablative regimen. Nonrelapse mortality did not differ according to regimen intensity. For patients aged 55 to 70 years, disease-free survival (HR, 0.97; 37% vs 43%; P = .83) and relapse (HR, 1.32; 42% vs 31%; P = .11) did not differ according to regimen intensity. Nonrelapse mortality was lower with reduced-intensity regimens (HR, 0.64; 20% vs 31%; P = .02). Myeloablative regimens are preferred for AML, ALL, and MDS; reduced-intensity regimens should be reserved for those unable to tolerate myeloablation.
Conflict of interest statement
Conflict-of-interest disclosure: The authors declare no competing financial interests.
Figures
References
-
- O’Donnell PV, Luznik L, Jones RJ, et al. Nonmyeloablative bone marrow transplantation from partially HLA-mismatched related donors using posttransplantation cyclophosphamide. Biol Blood Marrow Transplant. 2002;8(7):377-386. - PubMed
-
- Bashey A, Zhang X, Sizemore CA, et al. T-cell-replete HLA-haploidentical hematopoietic transplantation for hematologic malignancies using post-transplantation cyclophosphamide results in outcomes equivalent to those of contemporaneous HLA-matched related and unrelated donor transplantation. J Clin Oncol. 2013;31(10):1310-1316. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
