

Management of Difficult Tracheal Intubation: A Closed Claims Analysis
- PMID: 31584884
- PMCID: PMC6779339
- DOI: 10.1097/ALN.0000000000002815
Management of Difficult Tracheal Intubation: A Closed Claims Analysis
Abstract
Background: Difficult or failed intubation is a major contributor to morbidity for patients and liability for anesthesiologists. Updated difficult airway management guidelines and incorporation of new airway devices into practice may have affected patient outcomes. The authors therefore compared recent malpractice claims related to difficult tracheal intubation to older claims using the Anesthesia Closed Claims Project database.
Methods: Claims with difficult tracheal intubation as the primary damaging event occurring in the years 2000 to 2012 (n = 102) were compared to difficult tracheal intubation claims from 1993 to 1999 (n = 93). Difficult intubation claims from 2000 to 2012 were evaluated for preoperative predictors and appropriateness of airway management.
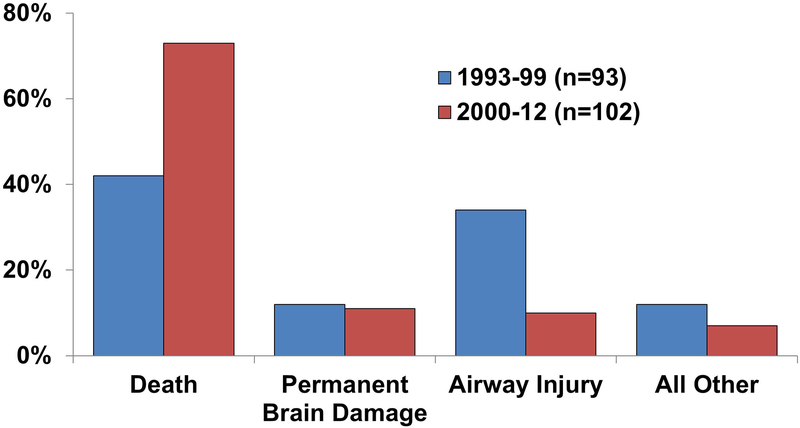
Results: Patients in 2000 to 2012 difficult intubation claims were sicker (78% American Society of Anesthesiologists [ASA] Physical Status III to V; n = 78 of 102) and had more emergency procedures (37%; n = 37 of 102) compared to patients in 1993 to 1999 claims (47% ASA Physical Status III to V; n = 36 of 93; P < 0.001 and 22% emergency; n = 19 of 93; P = 0.025). More difficult tracheal intubation events occurred in nonperioperative locations in 2000 to 2012 than 1993 to 1999 (23%; n = 23 of 102 vs. 10%; n = 10 of 93; P = 0.035). Outcomes differed between time periods (P < 0.001), with a higher proportion of death in 2000 to 2012 claims (73%; n = 74 of 102 vs. 42%; n = 39 of 93 in 1993 to 1999 claims; P < 0.001 adjusted for multiple testing). In 2000 to 2012 claims, preoperative predictors of difficult tracheal intubation were present in 76% (78 of 102). In the 97 claims with sufficient information for assessment, inappropriate airway management occurred in 73% (71 of 97; κ = 0.44 to 0.66). A "can't intubate, can't oxygenate" emergency occurred in 80 claims with delayed surgical airway in more than one third (39%; n = 31 of 80).
Conclusions: Outcomes remained poor in recent malpractice claims related to difficult tracheal intubation. Inadequate airway planning and judgment errors were contributors to patient harm. Our results emphasize the need to improve both practitioner skills and systems response when difficult or failed tracheal intubation is encountered.
Conflict of interest statement
Figures
Comment in
-
Current Difficult Airway Management-Not Good Enough!Anesthesiology. 2019 Oct;131(4):774-776. doi: 10.1097/ALN.0000000000002885. Anesthesiology. 2019. PMID: 31335551 No abstract available.
References
-
- Peterson GN, Domino KB, Caplan RA, Posner KL, Lee LA, Cheney FW: Management of the difficult airway: A closed claims analysis. Anesthesiology 2005; 103:33–9 - PubMed
-
- Hove LD, Steinmetz J, Christoffersen JK, Møller A, Nielsen J, Schmidt H: Analysis of deaths related to anesthesia in the period 1996–2004 from closed claims registered by the Danish Patient Insurance Association. Anesthesiology 2007; 106:675–80 - PubMed
-
- Cook TM, Scott S, Mihai R: Litigation related to airway and respiratory complications of anaesthesia: An analysis of claims against the NHS in England 1995–2007. Anaesthesia 2010; 65:556–63 - PubMed
-
- Fornebo I, Simonsen KA, Bukholm IRK, Kongsgaard UE: Claims for compensation after injuries related to airway management: A nationwide study covering 15 years. Acta Anaesthesiol Scand 2017; 61:781–9 - PubMed
-
- Cook TM, Woodall N, Frerk C; Fourth National Audit Project: Major complications of airway management in the UK: Results of the Fourth National Audit Project of the Royal College of Anaesthetists and the Difficult Airway Society. Part 1: Anaesthesia. Br J Anaesth 2011; 106:617–31 - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
