

Effect of a fluid bolus on cardiovascular collapse among critically ill adults undergoing tracheal intubation (PrePARE): a randomised controlled trial
- PMID: 31585796
- PMCID: PMC8852295
- DOI: 10.1016/S2213-2600(19)30246-2
Effect of a fluid bolus on cardiovascular collapse among critically ill adults undergoing tracheal intubation (PrePARE): a randomised controlled trial
Abstract
Background: Tracheal intubation is common in the care of critically ill adults and is frequently complicated by hypotension, cardiac arrest, or death. We aimed to evaluate administration of an intravenous fluid bolus to prevent cardiovascular collapse during intubation of critically ill adults.
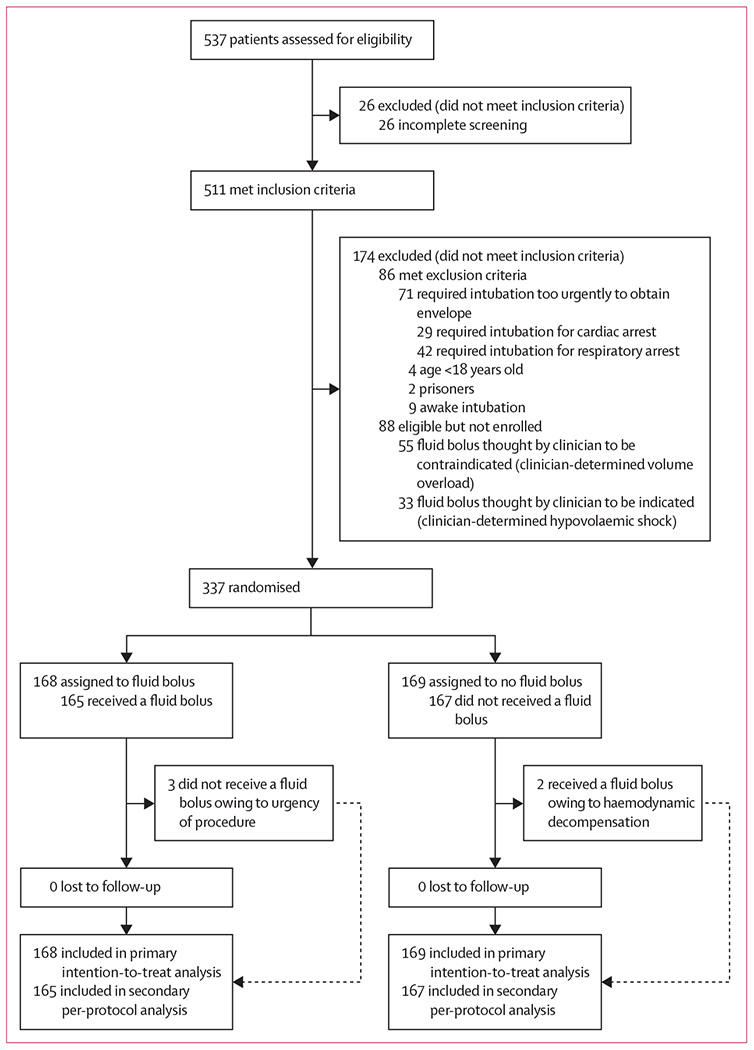
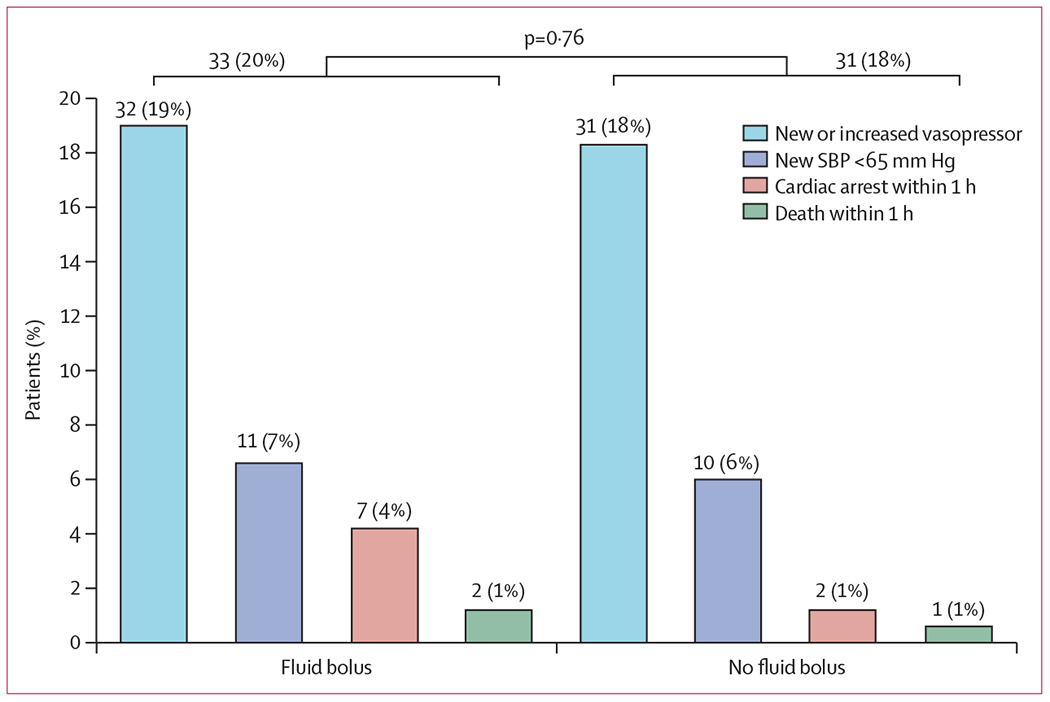
Methods: We did a pragmatic, multicentre, unblinded, randomised trial in nine sites (eight ICUs and one emergency department) around the USA. Critically ill adults (≥18 years) undergoing tracheal intubation were randomly assigned (1:1, block sizes of 2, 4, and 6, stratified by study site) to either an intravenous infusion of 500 mL of crystalloid solution or no fluid bolus. The primary outcome, assessed in the intention-to-treat population, was cardiovascular collapse, defined as a new systolic blood pressure <65 mm Hg; new or increased vasopressor receipt between induction and 2 min after tracheal intubation; or cardiac arrest or death within 1 h of tracheal intubation. Adverse events were assessed in the as-treated population. This trial, which is now complete, is registered with ClinicalTrials.gov, number NCT03026777.
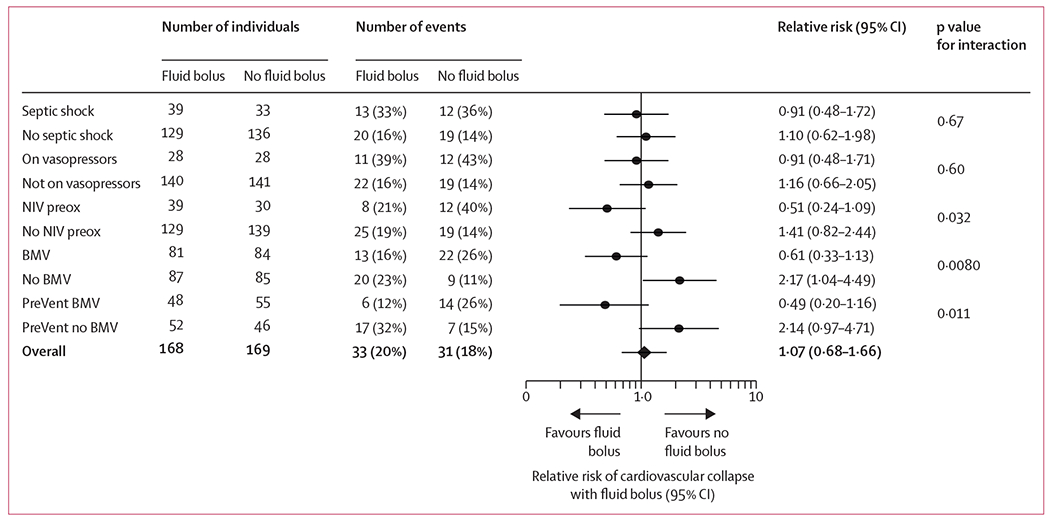
Findings: Patients were enrolled from Feb 6, 2017, to Jan 9, 2018, when the data and safety monitoring board stopped the trial on the basis of futility. By trial termination, 337 (63%) of 537 screened adults had been randomly assigned. Cardiovascular collapse occurred in 33 (20%) of 168 patients in the fluid bolus group compared with 31 (18%) of 169 patients in the no fluid bolus group (absolute difference 1·3% [95% CI -7·1% to 9·7%]; p=0·76). The individual components of the cardiovascular collapse composite outcome did not differ between groups (new systolic blood pressure <65 mm Hg 11 [7%] in the bolus group vs ten [6%] in the no-bolus group, new or increased vasopressor 32 [19%] vs 31 [18%], cardiac arrest within 1 h seven [4%] vs two [1%], death within 1 h of intubation two [1%] vs one [1%]). In-hospital mortality was not significantly different in the fluid bolus group (48 [29%]) compared with no fluid bolus (59 [35%]).
Interpretation: Administration of an intravenous fluid bolus did not decrease the overall incidence of cardiovascular collapse during tracheal intubation of critically ill adults compared with no fluid bolus in this trial.
Funding: US National Institutes of Health.
Copyright © 2019 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Rethinking rapid sequence induction of anaesthesia in critically ill adults.Lancet Respir Med. 2019 Dec;7(12):997-999. doi: 10.1016/S2213-2600(19)30275-9. Epub 2019 Oct 1. Lancet Respir Med. 2019. PMID: 31585797 No abstract available.
References
-
- Frat J-P, Thille AW, Mercat A, et al. High-flow oxygen through nasal cannula in acute hypoxemic respiratory failure. N Engl J Med 2015; 372:2185–96. - PubMed
-
- Jaber S, Jung B, Corne P, et al. An intervention to decrease complications related to endotracheal intubation in the intensive care unit: a prospective, multiple-center study. Intensive Care Med 2010; 36: 248–55. - PubMed
-
- Umobong EU, Mayo PH. Critical care airway management. Crit Care Clin 2018; 34: 313–24. - PubMed
-
- Green RS, Turgeon AF, McIntyre LA, et al. Postintubation hypotension in intensive care unit patients: a multicenter cohort study. J Crit Care 2015; 30:1055–60. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
