

Optimized Timing of Post-Transplantation Cyclophosphamide in MHC-Haploidentical Murine Hematopoietic Cell Transplantation
- PMID: 31586477
- PMCID: PMC7590501
- DOI: 10.1016/j.bbmt.2019.09.030
Optimized Timing of Post-Transplantation Cyclophosphamide in MHC-Haploidentical Murine Hematopoietic Cell Transplantation
Abstract
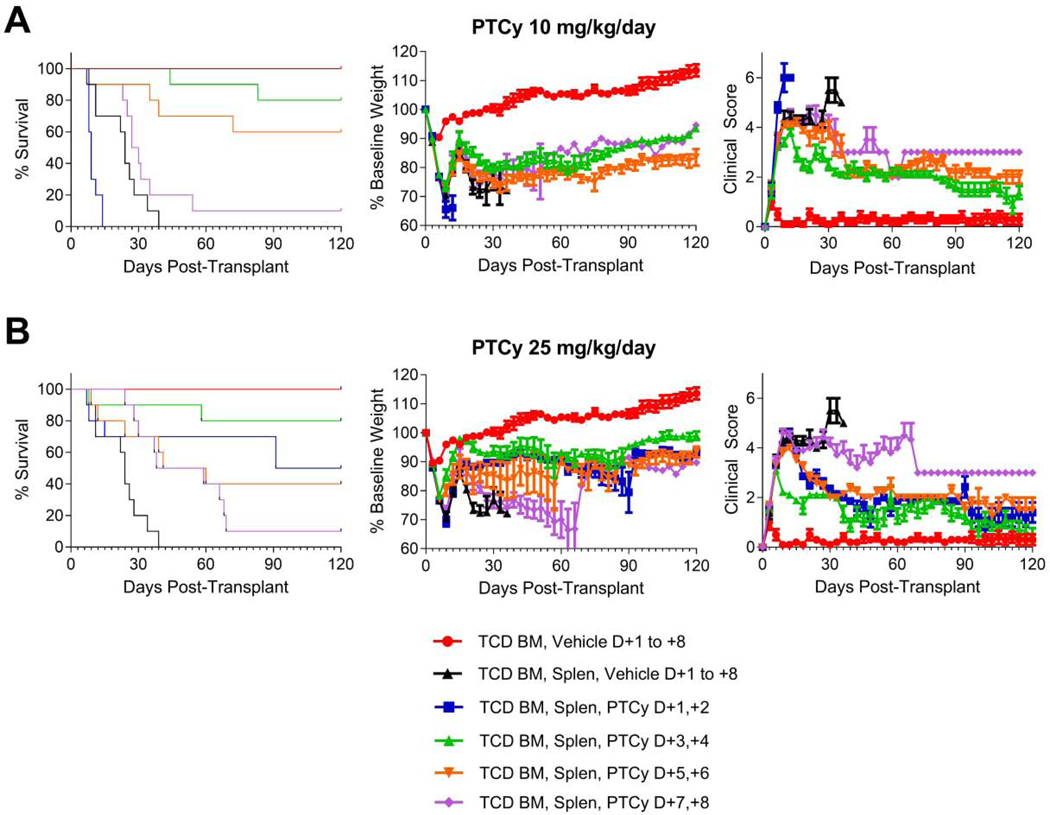
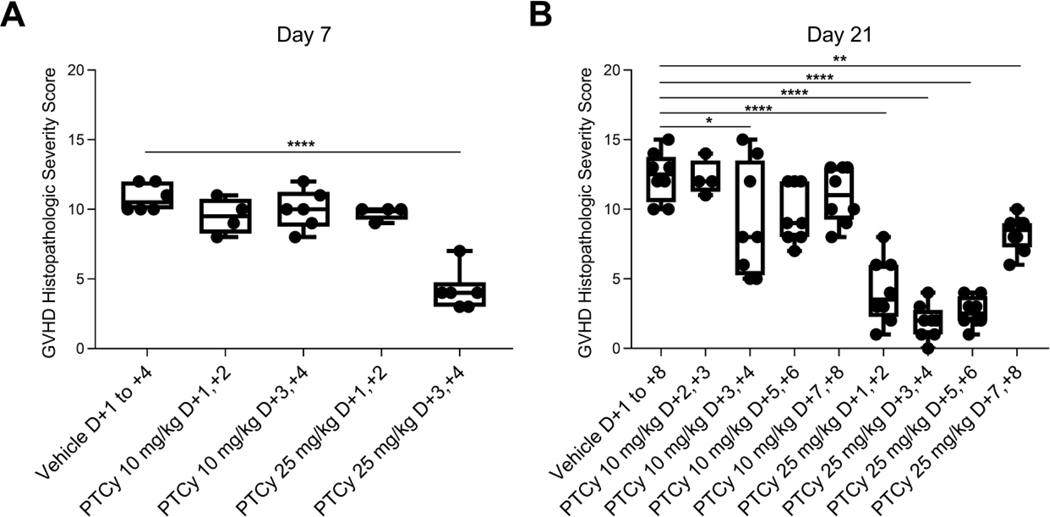
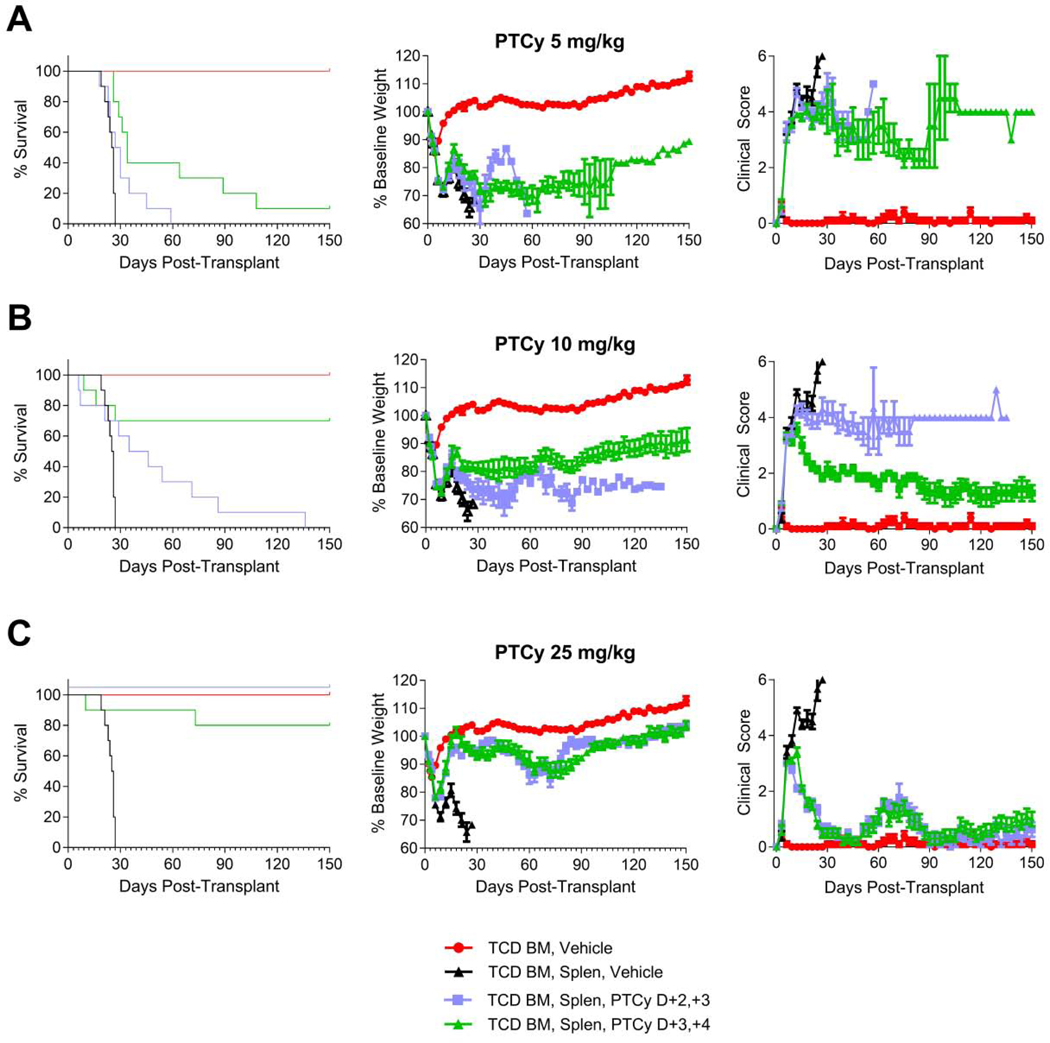
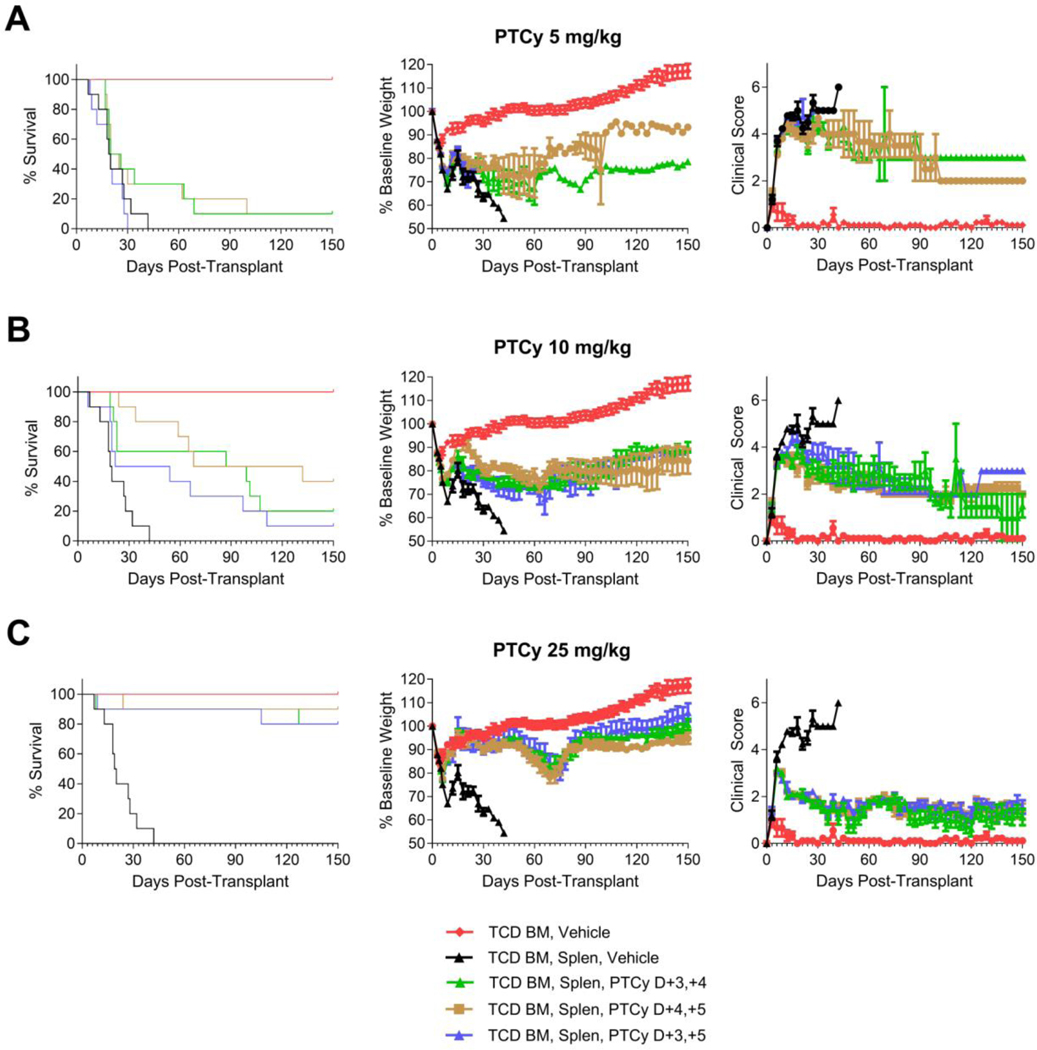
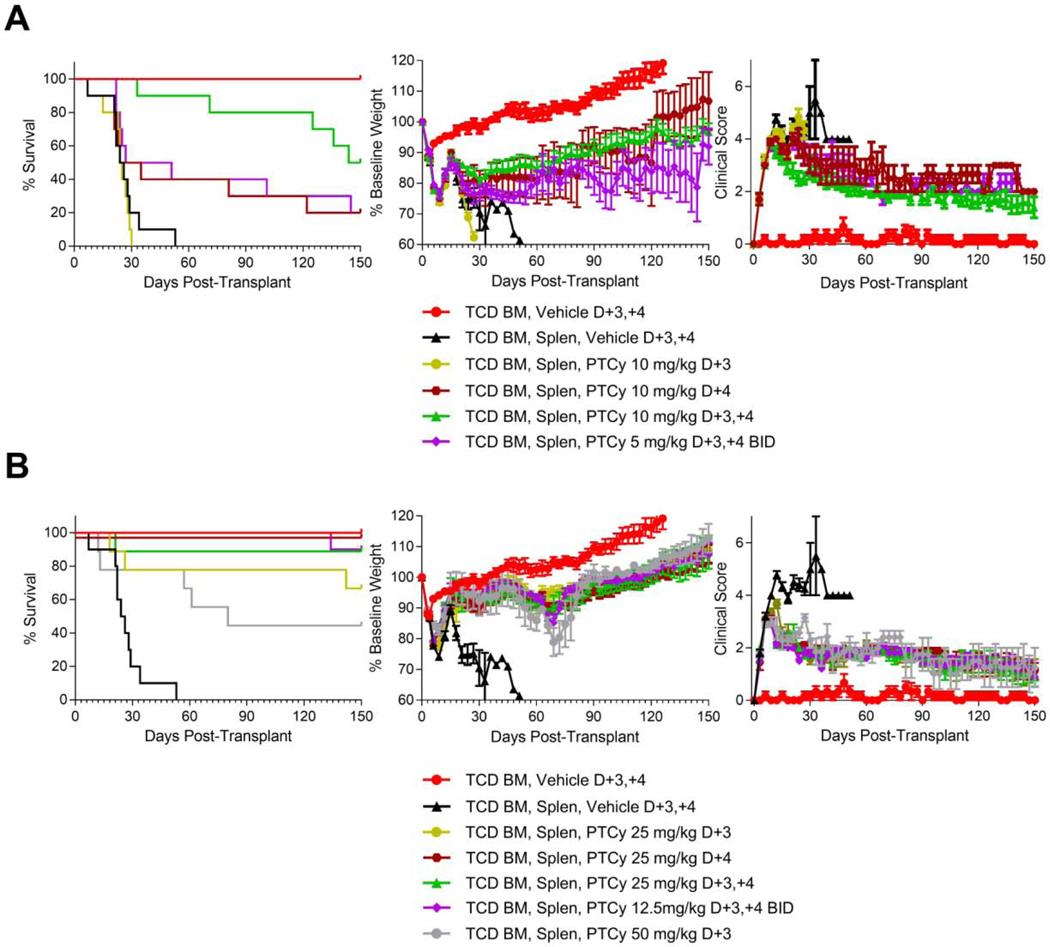
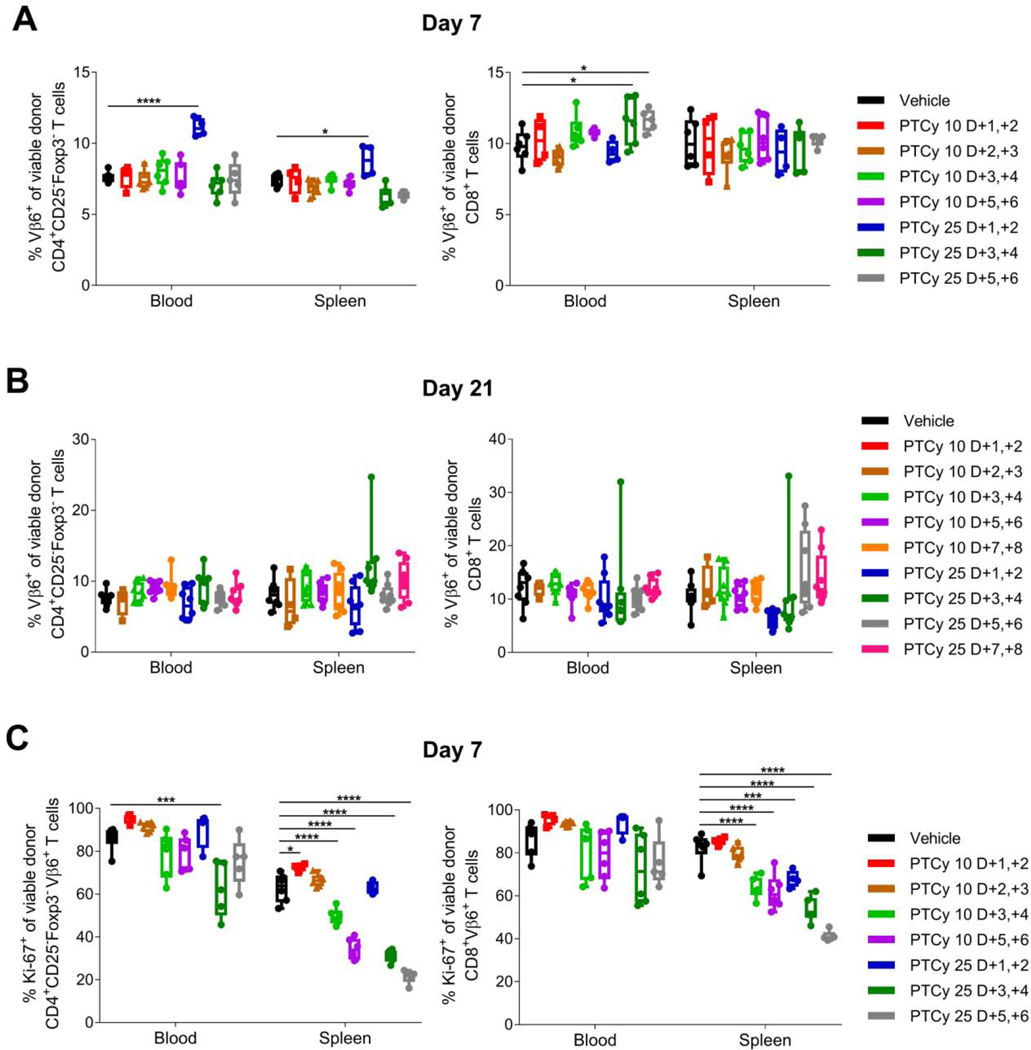
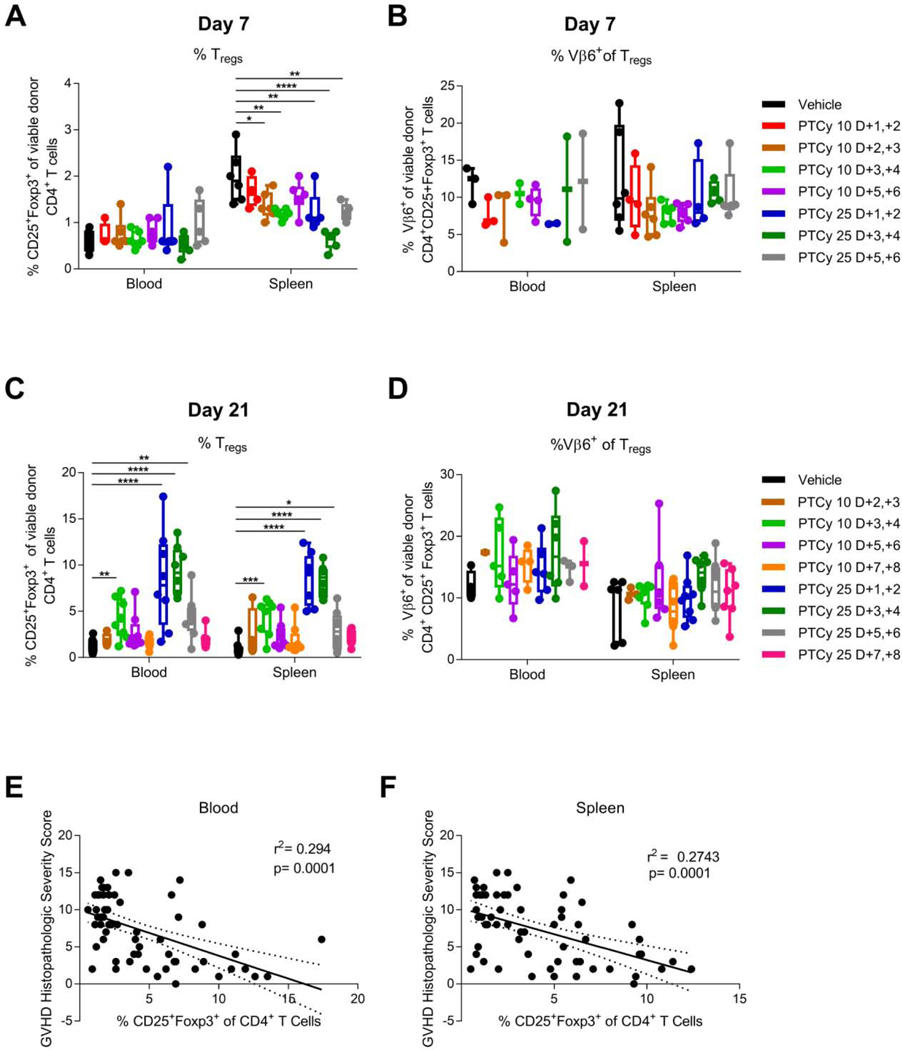
Post-transplantation cyclophosphamide (PTCy) reduces the risks of severe acute and chronic graft-versus-host disease (GVHD) after allogeneic hematopoietic cell transplantation (HCT). Yet, the standard clinical dose and timing of PTCy were partly extrapolated from MHC-matched skin allografting models and were partly empirical. Here we investigated the impact of differential dosing and timing of PTCy on its efficacy in preventing GVHD in a murine MHC-haploidentical HCT model. Administration of PTCy on days +3/+4 was superior to administration on days +1/+2, +5/+6, or +7/+8, whereas low-dose (10 mg/kg/day) PTCy on days +1/+2 actually led to accelerated death. Although the optimal timing of PTCy dosing was day +2 or +3 in the skin allografting models, in our MHC-haploidentical HCT model, PTCy on days +2/+3 was inferior to PTCy on days +3/+4 at lower doses. PTCy administered on days +3/+4, +4/+5, or +3/+5 were similarly efficacious. Single-day versus 2-day dosing schedules demonstrated that PTCy is maximally effective when given on day +4. Flow cytometric analysis showed that optimal PTCy dosing schedules both decreased alloreactive CD4+CD25-Foxp3- T cell proliferation at day +7 and allowed preferential CD4+CD25+Foxp3+ T cell reconstitution at day +21, suggesting that this combination may be a potential predictive biomarker of successful GVHD prevention by PTCy. These results show that the dose, timing, and cumulative exposure of PTCy all are critical for its efficacy in preventing GVHD. We are currently investigating the clinical relevance of these findings in a protocol seeking to optimize PTCy dose and timing and test these T cell endpoints as candidate biomarkers of successful GVHD prevention by PTCy.
Keywords: Alloreactive; Graft-versus-host disease; Haploidentical; Murine; Post-transplantation cyclophosphamide; Regulatory T cell.
Published by Elsevier Inc.
Conflict of interest statement
Figures
References
-
- Mayumi H, Himeno K, Tokuda N, Nomoto K. Drug-induced tolerance to allografts in mice. VII. Optimal protocol and mechanism of cyclophosphamide-induced tolerance in an H-2 haplotype-identical strain combination. Transplant Proc. 1986;18(2):363–369. - PubMed
-
- Luznik L, Jalla S, Engstrom LW, Iannone R, Fuchs EJ. Durable engraftment of major histocompatibility complex-incompatible cells after nonmyeloablative conditioning with fludarabine, low-dose total body irradiation, and posttransplantation cyclophosphamide. Blood. 2001;98(12):3456–3464. - PubMed
-
- Colson YL, Wren SM, Schuchert MJ, et al. A nonlethal conditioning approach to achieve durable multilineage mixed chimerism and tolerance across major, minor, and hematopoietic histocompatibility barriers. J Immunol. 1995;155(9):4179–4188. - PubMed
-
- Anasetti C, Amos D, Beatty PG, et al. Effect of HLA compatibility on engraftment of bone marrow transplants in patients with leukemia or lymphoma. N Engl J Med. 1989;320(4):197–204. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
