

Posttraumatic stress disorder increases the odds of REM sleep behavior disorder and other parasomnias in Veterans with and without comorbid traumatic brain injury
- PMID: 31587047
- PMCID: PMC7315766
- DOI: 10.1093/sleep/zsz237
Posttraumatic stress disorder increases the odds of REM sleep behavior disorder and other parasomnias in Veterans with and without comorbid traumatic brain injury
Abstract
Study objectives: To describe the crude prevalence of rapid eye movement (REM) sleep behavior disorder (RBD) following traumatic brain injury (TBI) and posttraumatic stress disorder (PTSD) in Veterans, given potential relationships between TBI, PTSD, RBD, and neurodegeneration.
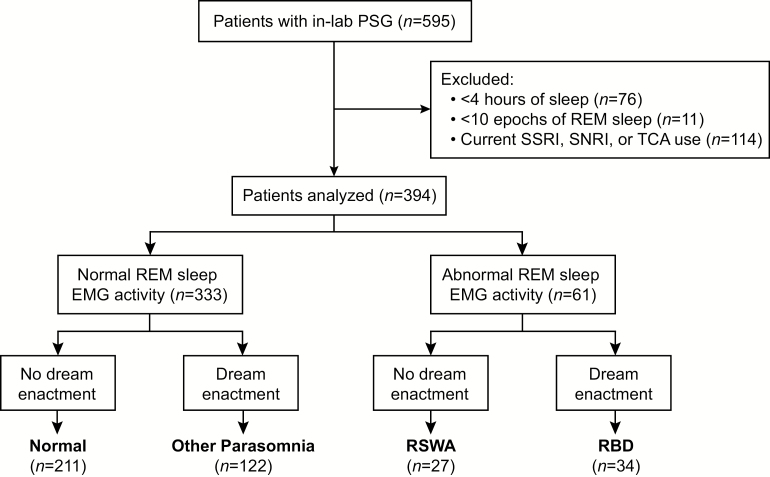
Methods: Veterans (n = 394; 94% male; 54.4 ± 15.5 years of age) were prospectively/cross-sectionally recruited from the VA Portland Health Care System and completed in-lab video-polysomnography and questionnaires. TBI and PTSD were assessed via diagnostic screening and medical record review. Subjects were categorized into four groups after assessment of REM sleep without atonia (RSWA) and self-reported dream enactment: (1) "Normal," neither RSWA nor dream enactment, (2) "Other Parasomnia," dream enactment without RSWA, (3) "RSWA," isolated-RSWA without dream enactment, and (4) "RBD," RSWA with dream enactment. Crude prevalence, prevalence odds ratio, and prevalence rate for parasomnias across subjects with TBI and/or PTSD were assessed.
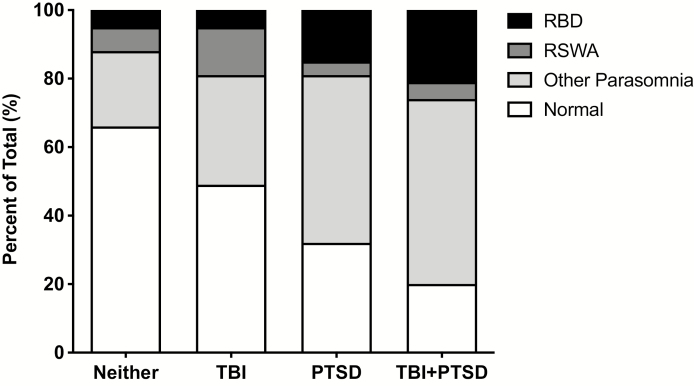
Results: Overall prevalence rates were 31%, 7%, and 9% for Other Parasomnia, RSWA, and RBD, respectively. The prevalence rate of RBD increased to 15% in PTSD subjects [age adjusted POR: 2.81 (1.17-4.66)] and to 21% in TBI + PTSD subjects [age adjusted POR: 3.43 (1.20-9.35)]. No subjects met all diagnostic criteria for trauma-associated sleep disorder (TASD), and no overt dream enactment was captured on video.
Conclusions: The prevalence of RBD and related parasomnias is significantly higher in Veterans compared with the general population and is associated with PTSD and TBI + PTSD. Considering the association between idiopathic-RBD and synucleinopathy, it remains unclear whether RBD (and potentially TASD) associated with PTSD or TBI + PTSD similarly increases risk for long-term neurologic sequelae.
Keywords: PTSD; RBD; REM sleep without atonia; TBI; trauma-associated sleep disorder.
Published by Oxford University Press on behalf of Sleep Research Society (SRS) 2019.
Figures
References
-
- Schenck CH, et al. .. Chronic behavioral disorders of human REM sleep: a new category of parasomnia. Sleep. 1986;9(2):293–308. - PubMed
-
- Dauvilliers Y, et al. . REM sleep behaviour disorder. Nat Rev Dis Primers. 2018;4(1):19. - PubMed
-
- Plazzi G, et al. . REM sleep behavior disorders in multiple system atrophy. Neurology. 1997;48(4):1094–1097. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
