

Medicines associated with dependence or withdrawal: a mixed-methods public health review and national database study in England
- PMID: 31588045
- PMCID: PMC7029276
- DOI: 10.1016/S2215-0366(19)30331-1
Medicines associated with dependence or withdrawal: a mixed-methods public health review and national database study in England
Abstract
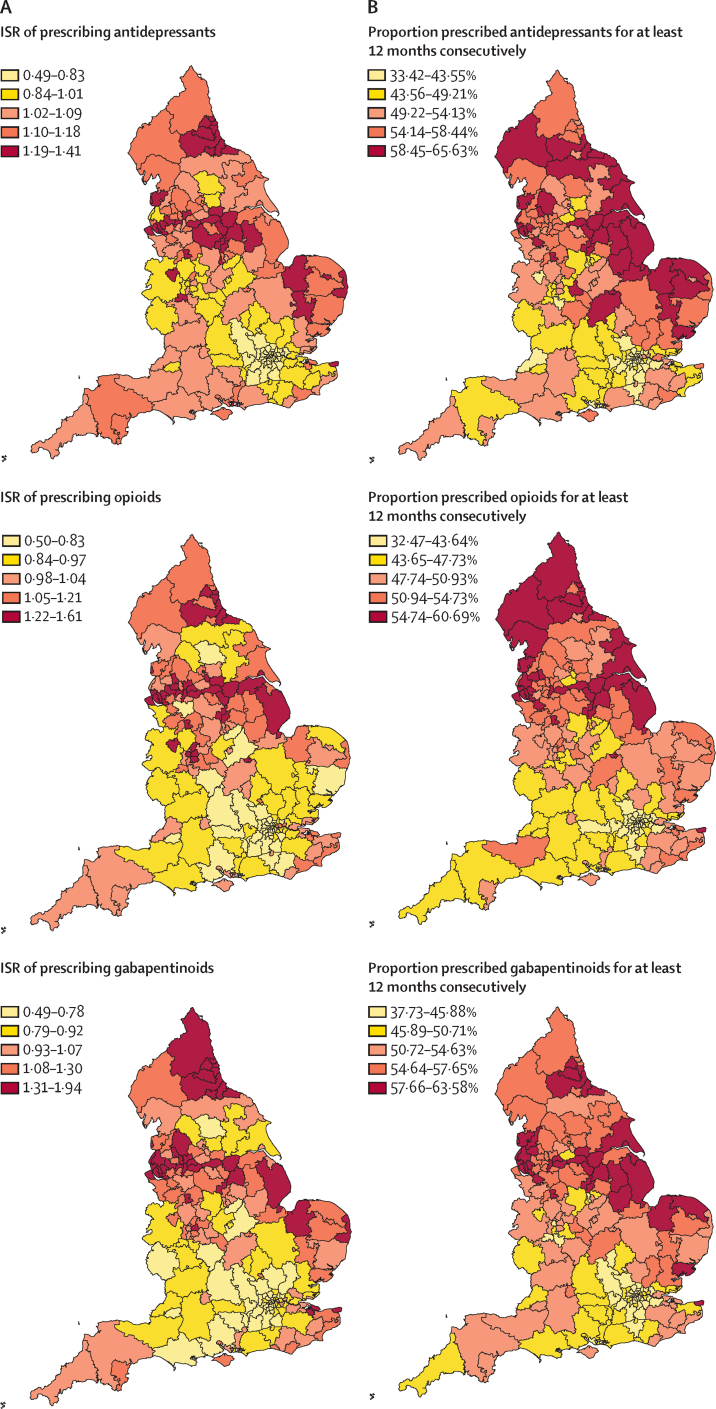
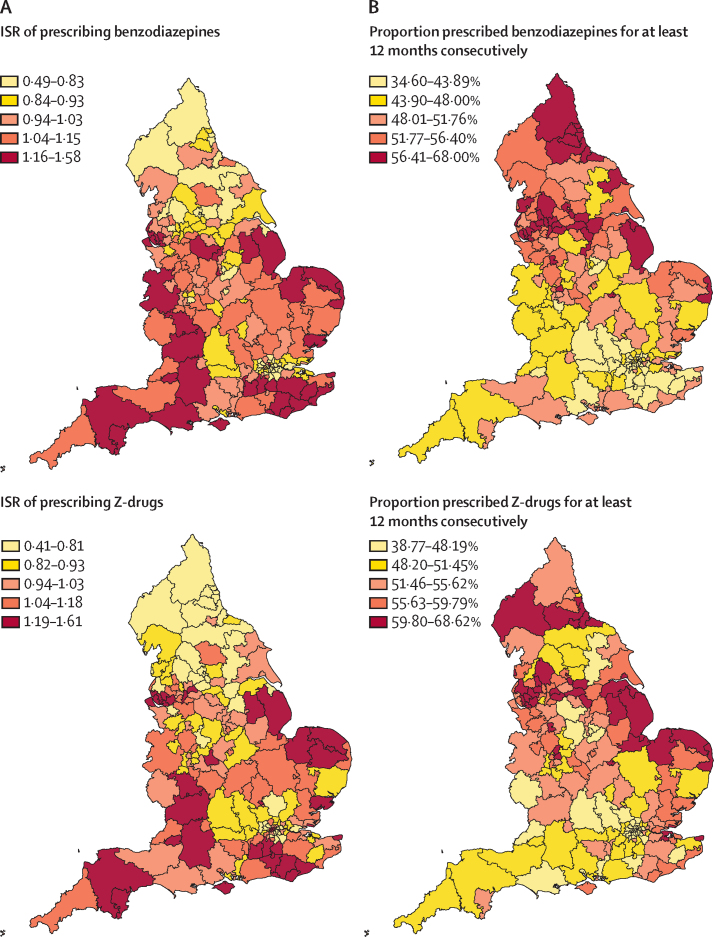
Background: Antidepressants, opioids for non-cancer pain, gabapentinoids (gabapentin and pregabalin), benzodiazepines, and Z-drugs (zopiclone, zaleplon, and zolpidem) are commonly prescribed medicine classes associated with a risk of dependence or withdrawal. We aimed to review the evidence for these harms and estimate the prevalence of dispensed prescriptions, their geographical distribution, and duration of continuous receipt using all patient-linked prescription data in England.
Methods: This was a mixed-methods public health review, comprising a rapid evidence assessment of articles (Jan 1, 2008, to Oct 3, 2018; with searches of MEDLINE, Embase, and PsycINFO, and the Cochrane and King's Fund libraries), an open call-for-evidence on patient experience and service evaluations, and a retrospective, patient-linked analysis of the National Health Service (NHS) Business Services Authority prescription database (April 1, 2015, to March 30, 2018) for all adults aged 18 years and over. Indirectly (sex and age) standardised rates (ISRs) were computed for all 195 NHS Clinical Commissioning Groups in England, containing 7821 general practices for the geographical analysis. We used publicly available mid-year (June 30) data on the resident adult population and investigated deprivation using the English Indices of Multiple Deprivation (IMD) quintiles (quintile 1 least deprived, quintile 5 most deprived), with each patient assigned to the IMD quintile score of their general practitioner's practice for each year. Statistical modelling (adjusted incident rate ratios [IRRs]) of the number of patients who had a prescription dispensed for each medicine class, and the number of patients in receipt of a prescription for at least 12 months, was done by sex, age group, and IMD quintile.
Findings: 77 articles on the five medicine classes were identified from the literature search and call-for-evidence. 17 randomised placebo-controlled trials (6729 participants) reported antidepressant-associated withdrawal symptoms. Almost all studies were rated of very low, low, or moderate quality. The focus of qualitative and other reports was on patients' experiences of long-term antidepressant use, and typically sudden onset, severe, and protracted withdrawal symptoms when medication was stopped. Between April 1, 2017, and March 31, 2018, 11·53 million individuals (26·3% of residents in England) had a prescription dispensed for at least one medicine class: antidepressants (7·26 million [16·6%]), opioids (5·61 million [12·8%]), gabapentinoids (1·46 million [3·3%]), benzodiazepines (1·35 million [3·1%]), and Z-drugs (0·99 million [2·3%]). For three of these medicine classes, more people had a prescription dispensed in areas of higher deprivation, with adjusted IRRs (referenced to quintile 1) ranging from 1·10 to 1·24 for antidepressants, 1·20 to 1·85 for opioids, and 1·21 to 1·85 for gabapentinoids across quintiles, and higher ISRs generally concentrated in the north and east of England. In contrast, the highest ISRs for benzodiazepines and Z-drugs were generally in the southwest, southeast, and east of England, with low ISRs in the north. Z-drugs were associated with increased deprivation, but only at the highest quintile (adjusted IRR 1·11 [95% CI 1·01-1·22]). For benzodiazepines, prescribing was reduced for people in quintiles 4 (0·90 [0·85-0·96]) and 5 (0·89 [0·82-0·97]). In March, 2018, for each of medicine class, about 50% of patients who had a prescription dispensed had done so continuously for at least 12 months, with the highest ISRs in the north and east. Long-term prescribing was associated with a gradient of increased deprivation.
Interpretation: In 1 year over a quarter of the adult population in England had a prescription dispensed for antidepressants, opioids (for non-cancer pain), gabapentinoids, benzodiazepines, or Z-drugs. Long-term (>12 months) prescribing is common, despite being either not recommended by clinical guidelines or of doubtful efficacy in many cases. Enhanced national and local monitoring, better guidance for personalised care, and better doctor-patient decision making are needed.
Funding: Public Health England.
Copyright © 2019 The Author(s). Published by Elsevier Ltd. This is an Open Access article under the CC BY-NC-ND 4.0 license. Published by Elsevier Ltd.. All rights reserved.
Figures
Comment in
-
Prescribing in primary care: art versus algorithm.Lancet Psychiatry. 2019 Nov;6(11):882-884. doi: 10.1016/S2215-0366(19)30373-6. Epub 2019 Oct 3. Lancet Psychiatry. 2019. PMID: 31588044 No abstract available.
References
-
- National Institute for Health and Care Excellence Medicines adherence: involving patients in decisions about prescribed medicines and supporting adherence. Clinical guideline [CG76] January, 2009. https://www.nice.org.uk/guidance/cg76
-
- Higgins C, Smith BH, Matthews K. Incidence of iatrogenic opioid dependence or abuse in patients with pain who were exposed to opioid analgesic therapy: a systematic review and meta-analysis. Br J Anaesth. 2018;120:1335–1344. - PubMed
-
- Chou R, Turner JA, Devine EB. The effectiveness and risks of long-term opioid therapy for chronic pain: a systematic review for a National Institutes of Health Pathways to Prevention Workshop. Ann Intern Med. 2015;162:276–286. - PubMed
-
- Berterame S, Erthal J, Thomas J. Use of and barriers to access to opioid analgesics: a worldwide, regional, and national study. Lancet. 2016;387:1644–1656. - PubMed
