

Male breast cancer in the United States: Treatment patterns and prognostic factors in the 21st century
- PMID: 31588557
- PMCID: PMC7668385
- DOI: 10.1002/cncr.32472
Male breast cancer in the United States: Treatment patterns and prognostic factors in the 21st century
Abstract
Background: Male breast cancer (MBC) is a rare disease for which there is limited understanding of treatment patterns and prognostic factors.
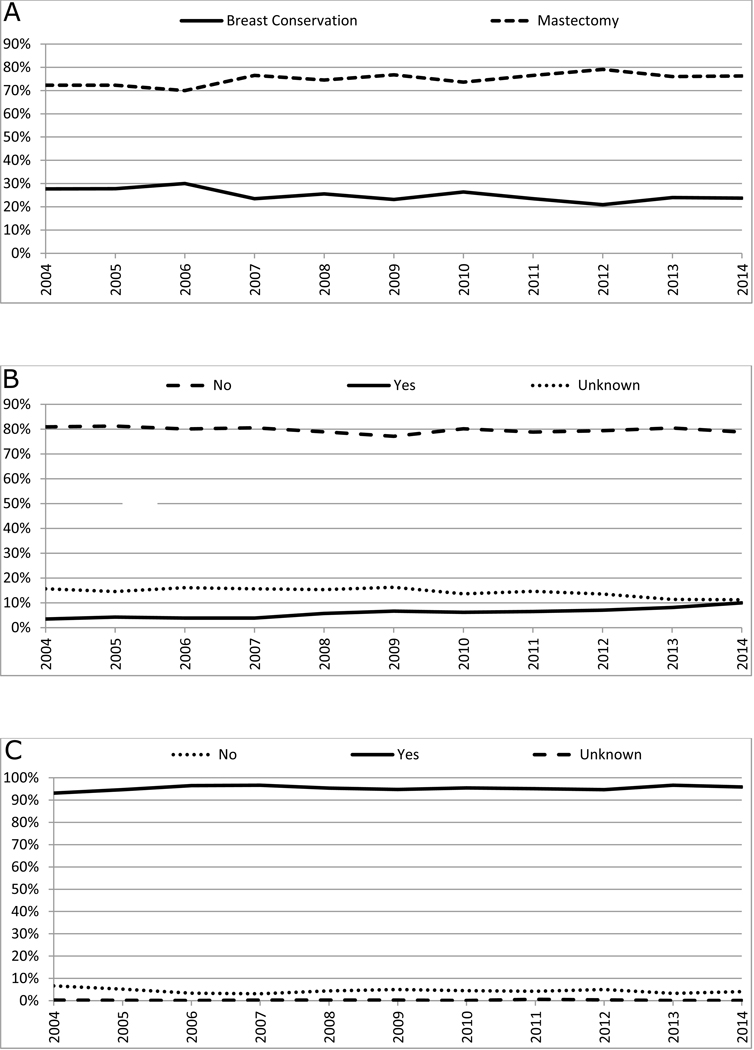
Methods: Men with TNM stage I to stage III breast cancer diagnosed between 2004 and 2014 in the National Cancer Data Base were included. Trends in treatment modalities were described using the average annual percentage change (AAPC) and estimated using Joinpoint software for the analysis of trends. Kaplan-Meier curves and the multivariate Cox proportional hazards regression model were used to compare survival between subgroups and to identify prognostic factors.
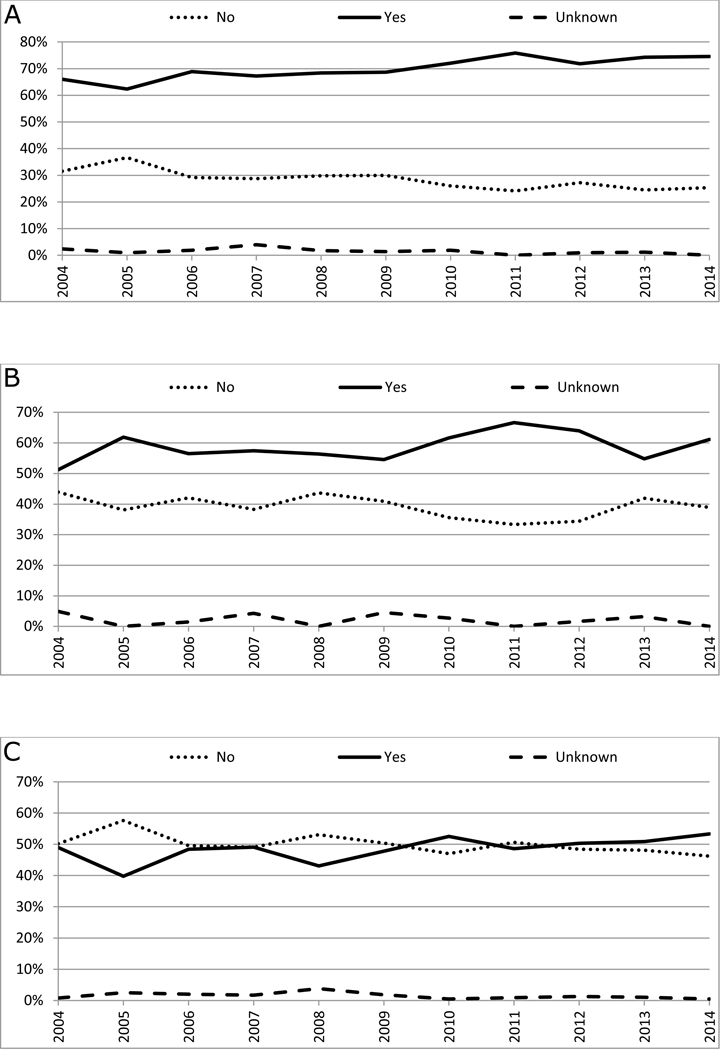
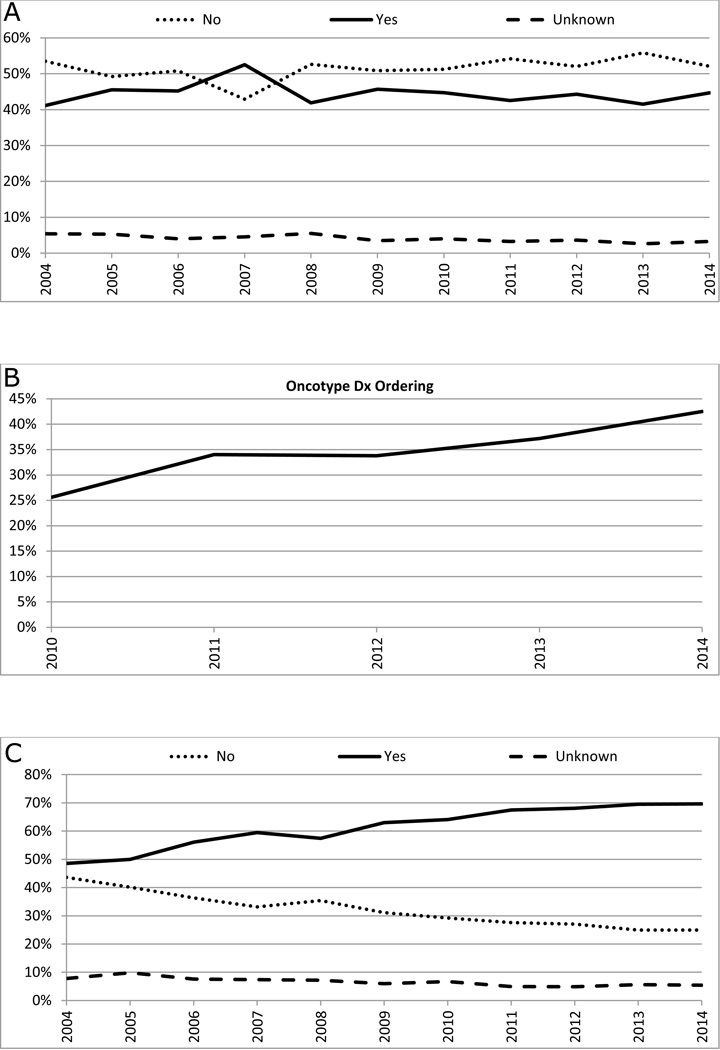
Results: A total of 10,873 MBC cases were included, with a median age at diagnosis of 64 years. Breast-conserving surgery was performed in 24% of patients, and 70% of patients undergoing breast conservation received radiotherapy. Approximately 44% of patients received chemotherapy, and 62% of patients with estrogen receptor-positive disease received endocrine therapy. Oncotype DX was ordered in 35% of patients with lymph node-negative, estrogen receptor-positive/human epidermal growth factor receptor 2 (HER2)-negative tumors. During the study period, there was a significant increase in the rates of total mastectomy, contralateral prophylactic mastectomy, radiotherapy after breast conservation, ordering of Oncotype DX, and the use of endocrine therapy (P < .05). On multivariate analysis, factors found to be associated with worse overall survival were older age, black race, higher Charlson Comorbidity Index, high tumor grade and stage of disease, and undergoing total mastectomy. Residing in a higher income area; having progesterone receptor-positive tumors; and receipt of chemotherapy, radiotherapy, and endocrine therapy were associated with better overall survival.
Conclusions: Despite the lack of prospective randomized trials in patients with MBC, the results of the current study demonstrated that the treatment of this disease has evolved over the years. These findings further the understanding of the modern treatment and prognosis of MBC, and identify several areas for further research.
Keywords: male; male breast cancer; pattern; survival; treatment; trend.
© 2019 American Cancer Society.
Conflict of interest statement
Figures
Comment in
-
Reply to On the proportion of male breast cancer among all breast cancers.Cancer. 2020 Jan 1;126(9):2034-2035. doi: 10.1002/cncr.32727. Epub 2020 Feb 3. Cancer. 2020. PMID: 32012222 Free PMC article. No abstract available.
-
On the proportion of male breast cancer among all breast cancers.Cancer. 2020 Jan 1;126(9):2034. doi: 10.1002/cncr.32731. Epub 2020 Feb 3. Cancer. 2020. PMID: 32012225 No abstract available.
-
The incidence of male breast cancer: from fiction to reality - correspondence.Int J Surg. 2023 Sep 1;109(9):2855-2858. doi: 10.1097/JS9.0000000000000512. Int J Surg. 2023. PMID: 37222665 Free PMC article. No abstract available.
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2018. CA Cancer J Clin. 2018;68: 7–30. - PubMed
-
- Noone AM HN, Krapcho M, Miller D, Brest A, Yu M, Ruhl J, Tatalovich Z, Mariotto A, Lewis DR, Chen HS, Feuer EJ, Cronin KA (eds). SEER Cancer Statistics Review, 1975–2015. Available from URL: https://seer.cancer.gov/csr/1975_2015/ [accessed December 4, 2018.
-
- Speirs V, Shaaban AM. The rising incidence of male breast cancer. Breast Cancer Res Treat. 2009;115: 429–430. - PubMed
-
- Anderson WF, Althuis MD, Brinton LA, Devesa SS. Is male breast cancer similar or different than female breast cancer? Breast Cancer Res Treat. 2004;83: 77–86. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
