

Simulation-based training is associated with lower risk-adjusted mortality in ACS pediatric TQIP centers
- PMID: 31589193
- PMCID: PMC6785206
- DOI: 10.1097/TA.0000000000002433
Simulation-based training is associated with lower risk-adjusted mortality in ACS pediatric TQIP centers
Abstract
Background: Although use of simulation-based team training for pediatric trauma resuscitation has increased, its impact on patient outcomes has not yet been shown. The purpose of this study was to determine the association between simulation use and patient outcomes.
Methods: Trauma centers that participate in the American College of Surgeons (ACS) Pediatric Trauma Quality Improvement Program (TQIP) were surveyed to determine frequency of simulation use in 2014 and 2015. Center-specific clinical data for 2016 and 2017 were abstracted from the ACS TQIP registry (n = 57,916 patients) and linked to survey responses. Center-specific risk-adjusted mortality was estimated using multivariable hierarchical logistic regression and compared across four levels of simulation-based training use: no training, low-volume training, high-volume training, and survey nonresponders (unknown training use).
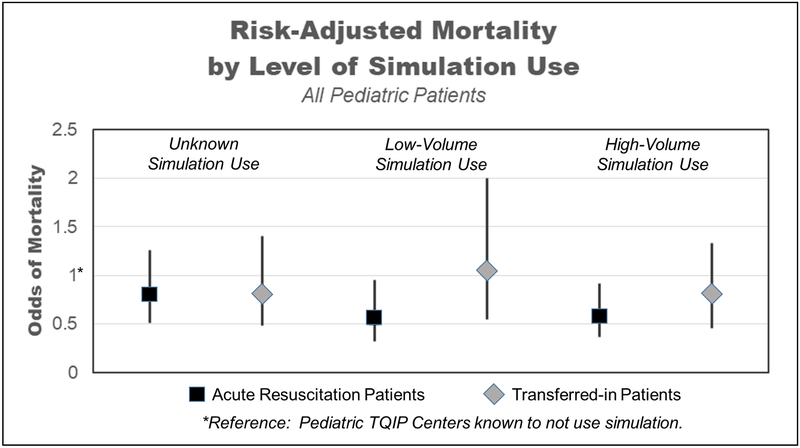
Results: Survey response rate was 75% (94/125 centers) with 78% of the responding centers (73/94) reporting simulation use. The average risk-adjusted odds of mortality was lower in centers with a high volume of training compared with centers not using simulation (odds ratio, 0.58; 95% confidence interval, 0.37-0.92). The times required for resuscitation processes, evaluations, and critical procedures (endotracheal intubation, head computed tomography, craniotomy, and surgery for hemorrhage control) were not different between centers based on levels of simulation use.
Conclusion: Risk-adjusted mortality is lower in TQIP-Pediatric centers using simulation-based training, but this improvement in mortality may not be mediated by a reduction in time to critical procedures. Further investigation into alternative mediators of improved mortality associated with simulation use is warranted, including assessment of resuscitation quality, improved communication, enhanced teamwork skills, and decreased errors.
Level of evidence: Therapeutic/care management, Level III.
Conflict of interest statement
None of the authors have any conflicts of interest to disclose. This work is not under consideration for publication in any other journal.
Figures
References
-
- Borse NN, Gilchrist J, Dellinger AM, Rudd RA, Ballesteros MF, Sleet DA. Unintentional childhood injuries in the United States: key findings from the CDC childhood injury report. J Saf Res. 2009;40:71–74. - PubMed
-
- National Center for Injury Prevention and Control, CDC using WISQARS. Ten Leading Causes of Death by Age Group, United States - 2015 Available from: https://www.cdc.gov/injury/wisqars/LeadingCauses.html. Accessed May 17, 2017.
-
- Potoka DA, Schall LC, Ford HR. Improved functional outcome for severely injured children treated at pediatric trauma centers. J Trauma. 2001;51:824–832; discussion 832-834. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
